Background: Pterygium is a sun-related ocular surface disease secondary to ultraviolet (UV) radiation exposure. Outdoor occupational UV exposure is known to occur secondary to sun exposure. We present a unique case of pterygium associated with indoor occupational light-emitting diode (LED) exposure not previously described in the literature.
Case Description: A mobile phone repairer presented with blurred vision and a superotemporal pterygium of his dominant left eye associated with a magnifying glass LED work lamp was diagnosed. This was excised routinely with conjunctival autografting to the defect. Histopathology confirmed benign pterygium and recovery was uncomplicated with resolution of blur.
Conclusions: The development of pterygium in our patient may have arisen due to the LED lamp’s wavelengths possibly falling within the UV as well as the upper end of the visible light radiation spectrum. Given the increasing reliance on LED light sources in modern life, ocular conditions arising from exposure to these radiation sources may now need to be listed in the differential diagnoses of patients with pterygium. Appropriate UV protection counselling for these types of lights may also now need to be considered.
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient for publication of this case report and the accompanying image. A copy of the written consent is available for review by the editorial office of this journal.
A 38-year-old man, employed as a mobile telephone repairer, was referred by his general practitioner with a suspected pinguecula in his left eye. He had noted slight vision disturbance on extreme left-gaze. Other than a recent infected insect bite above the left eyebrow 4 months prior, which was successfully treated with topical antibiotic ointment, he had no significant past ocular history. His medical history included gastro-oesophageal reflux and depression, managed with esomeprazole and fluoxetine, respectively.
The patient used an LED magnifying glass lamp directed from the temporal aspect of his left dominant eye, over an average of 30 hours per week for 16 months, to carry out precision mobile telephone repairs. He did not wear any occupational eye protection. The lamp was a Reichelt Elektronik LL ZD-2012B-2H 100 mm desk magnifying white glass lamp, which consisted of a glass lens with 3 dioptres, 1.75× magnification, with white LEDs arranged in a ring-shaped formation (5). The lamp had a colour temperature of 6,400 Kelvin (K) (5). He did not wear any occupational eye protection. The patient did not have a history of activities associated with beyond normal Australian sunlight exposure, such as surfing or truck-driving. There was no evidence of other ocular disorders such as trauma or chemical burn. Prior to mobile telephone repairs, his previous work was in warehouse logistics and did not involve use of UV lamps.
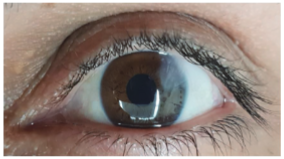
The patient’s visual acuity was 6/3.8 and intraocular pressures were 12 mmHg, both in each eye. Examination revealed a pterygium extending 4.25 mm radially into the cornea and with a base of 1.75 mm. It was triangular-shaped, located at the superotemporal aspect of the left eye (Figure 1), and just encroaching on the pupil margin with Ilse de Fuchs present at the apex. The rest of the ocular examination was within normal limits.
Figure 1 Slit lamp photograph of the left eye in primary position showing the supertemporal pterygium encroaching towards the pupil margin.
It is well reported that pterygium is a form of ‘ophthalmoheliosis’ that most commonly affects surfers and truck drivers (1). ‘Heliosis’, from Greek, refers to sun exposure and ‘ophthalmoheliosis’ are a group of ocular conditions arising from sun exposure. UV-A and UV-B radiations fall within the wavelengths of 315–400 nm and 280–315 nm respectively (6). UV-A and UV-B radiation are considered harmful and contribute to the pathogenesis of ocular surface and ocular media conditions including pterygium, pinguecula, and cataracts (6).
Our case of pterygium presumably associated with LED highlights the potential risks from either artificial source of UV LED radiation (7), or visible light radiation spectrum. The characteristics of UV radiation, including colour temperature and wavelength, are important features in the pathogenesis of pterygium (8).
The wavelengths of UV radiation are between 280–400 nm, and wavelengths of visible light are between 400–780 nm (6). Based on the principles of black body radiation, colour temperature is associated with a spectrum of wavelengths emitted by the black body radiation. The peak wavelength of the lamp, calculated using Wien’s displacement law and based on colour temperature of 6,400 K, was 450 nm. Thus, a wavelength of 450 nm falls just outside of UV radiation, within the visible light spectrum.
Short-wavelength (blue) LED light (464 nm) irradiation has also been reported to result in oxidative stress, activation of autophagy, and cell death (9). An in vivo mouse model has demonstrated that corneal epithelial apoptosis can be induced by blue LED exposure from the light source located 45 cm above them (10). Increased reactive oxygen species production, mitochondrial membrane damage and cell death in an immortalized human corneal epithelial cell line were also observed with blue LED light (10). The development of pterygium in our patient may thus have arisen as a result of the lamp’s wavelengths partially falling within the UV as well as the higher frequency violet end of the visible light radiation spectrum.
Occupations with considerable exposure (regarded as 38 hours per week) to sources of artificial UV radiation include watchmakers and welders (4). As our mobile phone repairer patient worked an average of 30 hours per week for 16 months with this LED lamp, his risk profile may warrant inclusion on this list.
Given the increasing reliance on LED light sources in modern life, ocular conditions arising from exposure to these radiation sources may need to be listed in the differential diagnoses of patients with pterygium. Appropriate UV protection counselling for these lights may also now need to be considered. As this is the first single observational case study to report on the potential harmful effect of LED emitted wavelengths, further case series studies, as a minimum, are needed to confirm this finding as causative.
Reporting Checklist: The authors have completed the CARE reporting checklist. Available at https://aes.amegroups.com/article/view/10.21037/aes-22-8/rc
Peer Review File: Available at https://aes.amegroups.com/article/view/10.21037/aes-22-8/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://aes.amegroups.com/article/view/10.21037/aes-22-8/coif). KGJO serves as an unpaid editorial board member of Annals of Eye Science from December 2021 to November 2023. SLW is supported by a Sydney Medical School Foundation fellowship. The other author has no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient for publication of this case report and the accompanying image. A copy of the written consent is available for review by the editorial office of this journal.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.









