Cataract is one of the common causes of vision impairment among the elderly. It is a metabolic disorder that affects the lens of eyes due to multiple factors, leading to degeneration and turbidity of the lens protein, reducing the amount of light reaching the retina, resulting in blurred vision (1). Currently, the extraction of cataract is the only effective measure to treat cataract, which is the world’s first blinding eye disease (2). Daytime surgery refers to the surgery performed on a patient in one working day after admission, surgery and discharge, except for outpatient operations performed in physicians’ clinics or hospitals (3). As daytime surgery is being increasingly improved, patients’ requirements for medical efficacy and the quality of medical services are also growing. Due to the heavy workload of medical staff in cataract ward and the batch work flow, all patients return to the inpatient ward on the 1st day after surgery and wait for the physician’s examination before going through the discharge formalities, resulting in a crowded and noisy environment around the ward and the hospital billing office. The long waiting time for the elevator and the discharge settlement leads to the patients’ dissatisfaction with the quality of medical services and even the waste of some human and material resources. Therefore, there is an urgent need to remodel the entire set-up of handling the outnumbered patients coming for same day surgery and discharge. However, it remains a key issue regarding how to establish an efficient and orderly discharge process on the day of operation using effective resources. To further improve overcrowding to increase patients’ satisfaction, and awareness rate of health education, we set-up the entire discharge procedure on the day of operation within the department. The clinical effects and outcomes of the improvement are discussed in this paper.
We present the following article in accordance with the STROBE checklist (available at http://dx.doi.org/10.21037/aes-20-78).
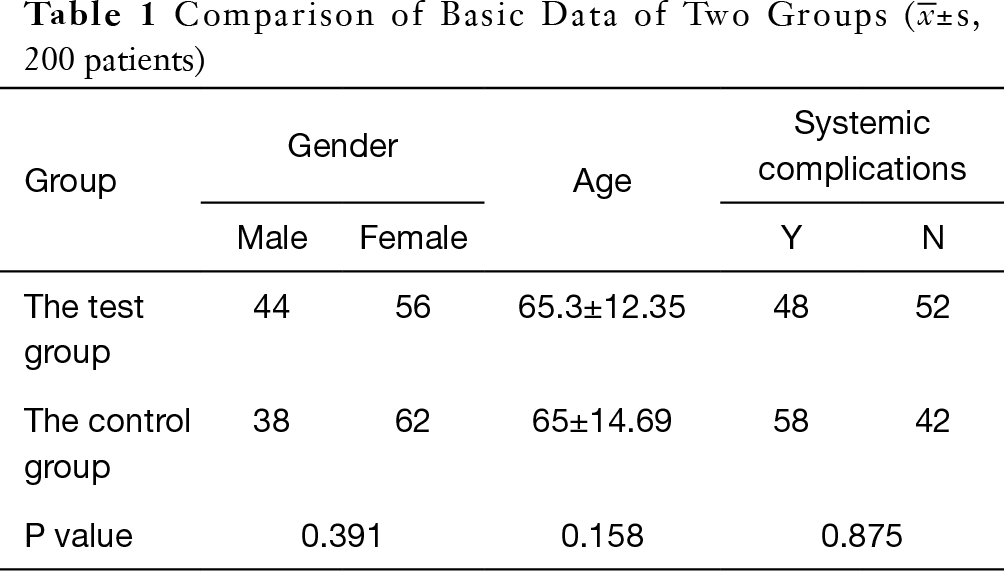
In this study, 200 patients undergoing daytime surgery were admitted to the cataract Ward from August 2019 to January 2020. The cataract phacoemulsification combined with intraocular lens implantation was performed in the surgical method. The selection criteria were: conformation of the patients to the diagnostic criteria of clinical cataract surgery; the time of hospitalization should not be more than 24 hours; Patients with clear consciousness, who can’t cooperate with the investigation. Exclusion criteria: patients with consciousness disorder who can’t cooperate with the investigation. 200 patients were divided into groups according to the time of admission, and 100 patients admitted to hospital in August 2019 were selected as the control group, and 100 patients admitted to hospital in January 2020 were used as the test group to avoid information contamination caused by the simultaneous operation of the two groups. The control group included 38 males and 62 females with an average age of (65±14.69) years; The experimental group included 44 males and 56 females with an average age of (65.3±12.35) years. The basic data of the two groups showed no statistical significance (P>0.05) and were comparable, as shown in Table 1. As the instructions of the relevant departments of our hospital, this study is no ethics involved, therefore, the ethical approval process is not needed. Informed consent was taken from all patients.
For the control group, the routine mode of discharge process was implemented, i.e., the preoperative examination was completed in the outpatient pre-admission department under the supervision of a specialist, the perioperative nursing care was provided according to the severity of the cataract on the day of admission. The patients were observed for half an hour after the operation in the operating room. None of the patients reported any signs of discomfort, so they were allowed to leave the hospital with their family members. The next morning, the patients returned to the inpatient ward to finish the discharge formalities after their follow-up with the physician.
For the experimental group, similar routine mode of discharge process was optimized, to facilitate the patients to seek better medical treatment. The discharge process mode was implemented on the day of operation, i.e., the preoperative examination was completed in the outpatient pre-admission department under the supervision of a specialist, the perioperative nursing care was provided according to the severity of the cataract on the day of admission, the patients were closely monitored for any discomfort after the surgery in the operating room for half an hour. If they did not show any signs of discomfort, they were allowed to go to the discharge directly and did not have to wait until the next day. The next morning, the patients returned to the outpatient and to follow-up with the physician. The specific implementation methods were as follows:
With the coordination of the Information Department and the Medical Department, a postoperative review guide sheet was printed in the inpatient system. All are patient-centered. As per the operation time of the patients in the ward, the working hours for the inpatient billing office and pharmacy were negotiated, and the issue of repeated queuing for payment was tackled. A medicine picks up window for patients in the cataract ward was set up, and the payment list was made and the nursing staff were asked to remind the patient of any due payments the next day.
Physicians were required to document all the medical records of the patients at the time of their discharge. The nursing staff helped the patients in the post-operation observation room in handling the discharge process and to remind them of their follow-up the next day at 7:30 am for re-examination.
Compared to the previous implementation, a lots of work load on part of the nursing staff was reduced. Since, the operations performed on the patients in cataract ward varied every day, the job responsibilities of the staff were adjusted, shifts were rearranged as per the requirements, human resources were properly allocated, and work hours were flexible and subjected to the actual situation.
As the length of hospital stay for patients was shortened, to make patients more familiar with the process, nurses were required to strengthen their communication abilities with patients, expand their efforts in spreading health education, deepen their professional knowledge in spare time, improve their professional quality, enhance their sense of responsibility, and become familiar with the new work process, thus making the work more organized and them fully capable of completing the work efficiently and accurately.
To relieve the pressure resulted from large batches of patients in the ward, and to avoid the long waiting time for the elevator, patients were grouped into batches and were sent to the outpatient clinic for re-examination on the next day post-operation. The nurses assisted in removing the eye bags, cleaning the eye circumference, measuring intraocular pressure, maintaining order, and guiding the patients to the corresponding position at the entrance of the clinic for the physicians’ examinations.
To ensure that patients can directly contact the ward if their condition is worsened or is critical, a 24-hour ward contact phone number was available. The treatment process for discharged patients, the emergency treatment process, and the medication process for postoperative conditions, etc. were delayed.
(I) Length of stay, waiting time for elevator, hospitalization expenses.
(II) Patient satisfaction: A self-made scale was used to investigate patient satisfaction, involving 9 items, each of which was rated as satisfactory, average and unsatisfactory. Likert-3 scoring method was used, with a full score of 18 points and 15 points or more as satisfactory.
(III) Awareness rate of health education: The self-made scale was used to investigate the awareness rate of health education in patients, including 15 items, each of which was rated as awareness, partial awareness and non-awareness, with a full score of 30 points and 27 points and more being awareness.
SPSS19. 0 was used for statistical analysis. The counting data were tested by χ2 test and described by No. of patients (%); Measurement data were tested by t and described by (
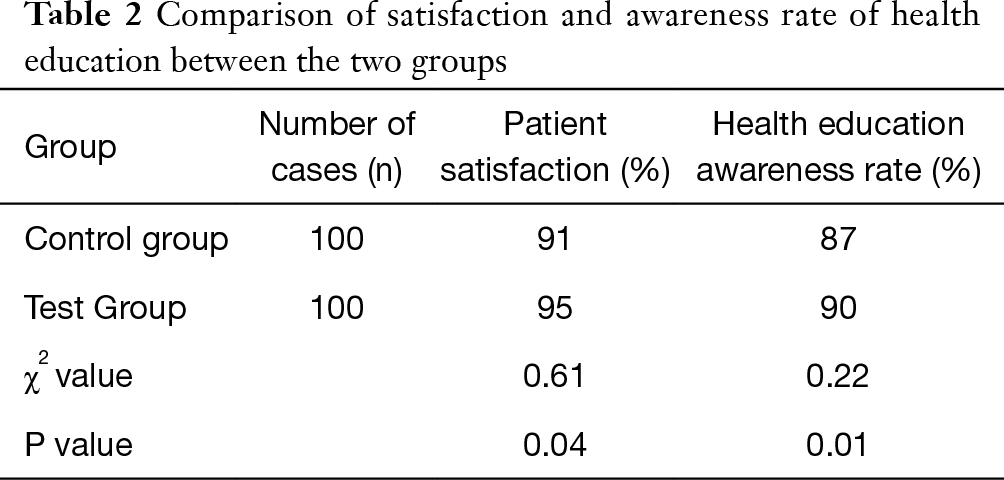
Comparison of satisfaction and awareness rate of health education between the two groups The patients’ satisfaction rate increased from 91% to 95%, and the rate of awareness of health education increased from 87% to 90%, the difference was statistically significant (χ2=0.61, P=0.04 and χ2=0.22, P=0.01; Table 2).
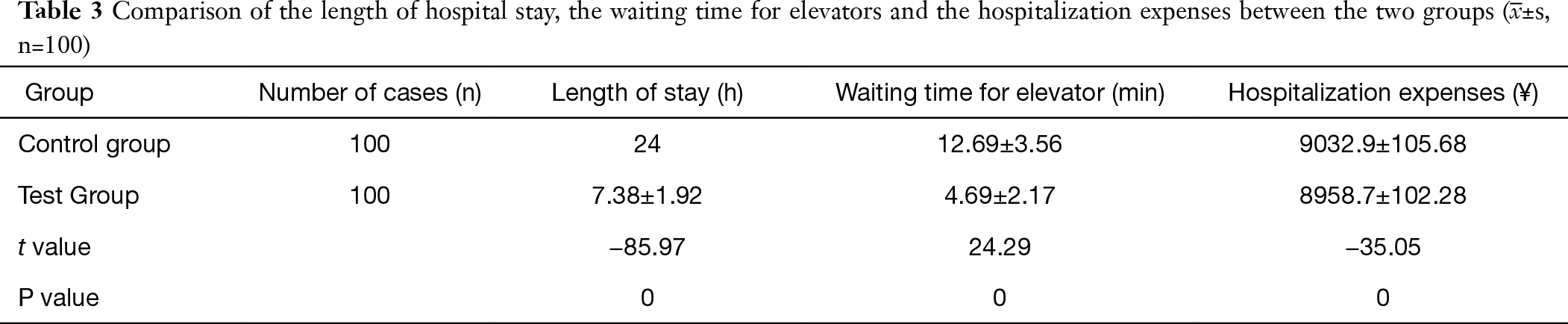
Comparison of the length of hospital stay, the waiting time for elevators and the hospitalization expenses between the two groups The results of this survey suggested that the length of hospital stay, the waiting time for elevators and the hospitalization expenses were notably lower than before implementation of the set-up, the difference was statistically significant(t=–85.97, 24.29, –35.05, P=0; Table 3).
With the implementation of daytime surgery, the current situation of “difficulty and expensive medical service” for patients, has been alleviated to a certain extent. However, because of the convenience of daytime surgery that postoperative care is performed by patients and their families at home. Some studies indicate that 40.9% of patients worry about the lack of their medicare knowledge, whilst more than half of the patients and their families worry about their incapability to deal with any complications at home, that could suffice post-operation (4). Based on the large operation volume and batch workflow, it is hard to ensure patient satisfaction and awareness rate of health education. Therefore, there is an urgent need for the hospital management to deal with proper allocation of the medical staff, improving work efficiency and reducing the cost of the entire process (5).
There has been a shortage of the medical and nursing staff in the cataract ward, and the workload of the nurses is heavy, thereby creating a lot of psychological pressure in them. After the discharge mode is implemented on the day of operation, the workload of nurses is reduced as compared to pre-implementation, thus improving the workload and motivation of the nursing staff to work efficiently. The patients are sent to the outpatient department in batches for re-examination the next day post-operation, so that physicians can identify and examine patients quickly and the crowding of new and old patients in the ward can be avoided, thereby ensuring a smooth and orderly ward workload and a proper and efficient use of medical and nursing staff.
Through optimisation of the discharge process on the day of operation, the length of hospital stays and waiting time for elevators are shortened, and the patients were prevented from showing up a number of times, which improves the patient satisfaction. With a significant reduction in the work load of the nursing staff, they are able to help in spreading health education and improving the awareness rate of health education of the patients in order to make the patients more familiar with the entire new set-up. Although the opening of a 24-hour helpline alleviates the psychological pressure and the anxieties of patients, it also ensures a timely treatment provided to the patients by the medical staff to save their lives.
The results of this study show that since the discharge mode of cataract patients on the day of operation, the efficiency of medical staff has been improved without increasing the human resources of medical staff. However, due to different hospital, different department management mode, personnel structure, hospital culture, the improvement measures may also be different (6). Therefore, the results obtained in this study suggest that managers should draw lessons from the clinical practice.









