Abstract: Advances in intraocular lens (IOL) design have rendered cataract surgery a refractive procedure. Newer IOL types include bifocal, trifocal and extended depth of focus (EDOF) IOLs. Their basic difference nestles in the number of focal points that each lens provides, which in turn leads to different visual outcomes. Familiarity of surgeons with the various characteristics of each lens is of utmost importance for accurate IOL selection to match each patient’s needs. In this review, we aim to compare the clinical outcomes after implantation of multifocal and EDOF IOLs in terms of distance, intermediate and near vision, contrast sensitivity, and reading performance. Finally, we discuss the defocus curve and the optical and photic phenomena associated with each type of IOL.
Cataract is one of the leading causes of vision impairment on a global scale. The goal of cataract surgery is to restore vision by replacing the opacified crystalline lens with an artificial intraocular lens (IOL). However, in recent years advances in IOL technology have attributed to cataract surgery the status of a refractive procedure (1). Thus, the new goal of cataract surgery has transitioned from restoring vision to offering spectacle independence (2). A key component in this transition has been the development of multifocal IOLs. Multifocal IOLs are designed to split light into different foci, using either refractive or diffractive optics (3).
The most commonly used multifocal IOLs are the bifocal ones, which create two primary focal points, one for distance and one for near vision (4). The insufficient intermediate vision that these lenses offer has been one of their main drawbacks, especially due to the expanding needs of modern-day patients (e.g., use of electronic devices etc.) (5). Trifocal IOLs were, thus, subsequently introduced, offering a third focal point for intermediate vision. However, the greater division of light that occurs as it passes through a trifocal IOL is also responsible for the optical phenomena (e.g., glare and halos) and the loss of contrast sensitivity that occurs after implantation of such IOLs (6). In an attempt to achieve good quality of vision at all distances, while avoiding undesirable photic phenomena, a new generation of IOLs was introduced, the extended depth of focus (EDOF) IOLs. The EDOF technology is based on the elongation of the distance the eye remains in focus, thus aiming to provide an uninterrupted range of vision (3,7).
This review article offers a comprehensive overview of the visual performance of bifocal, trifocal and EDOF IOLs, in terms of visual acuity, contrast sensitivity, reading ability and optical phenomena. The pros and cons of each type of IOL are summarized in Table 1.
| Type of IOL | Distance vision | Intermediate vision | Near vision | Reading performance | Contrast sensitivity | Optical phenomena |
|---|---|---|---|---|---|---|
| Bifocal IOLs | +++ | + | +++ | +++ | +++ | +++ |
| Trifocal IOLs | +++ | +++ | +++ | +++ | ++ | ++ |
| EDOF IOLs | +++ | +++(+)* | ++ | +++ | +++ | ++ |
A (+) sign indicates performance of the IOL in terms of vision, reading performance and contrast sensitivity. The more (+) signs indicate higher performance. In case of optical phenomena more (+) signs indicate higher frequency of optical phenomena. *, EDOF IOLs outperform trifocal IOLs in terms of intermediate vision under mesopic conditions, but they exhibit similar results under photopic conditions. EDOF, extended depth of focus; IOL, intraocular lens.
Trifocal lenses were developed in order to ameliorate the quality of intermediate vision through the incorporation of a third focal point that bifocal IOLs lacked. Several studies have investigated whether implantation of trifocal IOLs held its promise to improve intermediate vision compared to bifocal IOLs. Liu et al. (4) conducted a prospective, non-randomized study enrolling 55 patients, 30 of which underwent implantation of the diffractive bifocal IOL AT LISA 809M (Carl Zeiss Meditec, Jena, Germany) and the remaining 25 of the trifocal IOL AT LISA tri 839MP (Carl Zeiss Meditec, Jena, Germany). After a follow-up period of 3 months, the near and distance vision were measured, showing no statistical difference (P>0.05). On the other hand, the uncorrected intermediate visual acuity (UIVA) measured at 80 cm was significantly better in the trifocal IOL group (mean: 0.08 logMAR or 20/25 in UIVA) compared to the bifocal IOL group (mean: 0.26 logMAR or 20/40 in UIVA) (all P<0.01) (4).
A better visual outcome, as far as intermediate vision is concerned, was also observed in the studies of Gundersen et al. (8) and Mojzis et al. (9), who pointed out the superiority of the trifocal lens AT LISA tri 839MP at ?0.50, ?1.00 and ?1.50 D when compared to the ReSTOR SV25T0/SN6AD1 (Alcon Laboratories, Inc., Fort Worth, TX, USA) and the AT LISA 801 (Carl Zeiss Meditec, Jena, Germany) bifocal IOLs, respectively. Finally, Brezna et al. (10) highlighted the importance of luminosity in measuring the visual acuity with bifocal or trifocal lenses. Unfortunately, there is no international agreement on luminosity settings and such visual acuity measurements can lead to inaccurate conclusions.
The newest advent in IOL development are EDOF, also referred to as extended range of vision (ERV), IOLs which have the ability to create a continuum of foci through the implementation of spherical aberration and the presence of optically active transitional zones (11). Consequently, an extended area of focus is created, enhancing the quality of intermediate vision (12). The Tecnis Symfony (Abbott Medical Optics, Inc., Abbott Park, IL, USA) was the first EDOF-labeled IOL approved by the U.S. Food and Drug Administration in 2016 (13). Since then, numerous studies have been conducted, comparing the EDOF lenses mainly to the trifocal IOLs, as well as to the bifocal ones.
EDOF lenses exhibit similar results in terms of distance vision when compared to trifocal or bifocal IOLs. More specifically, Cochener et al. (3) reported no statistically significant difference between the EDOF lens Tecnis Symfony and the trifocal lenses AcrySof IQ PanOptix (Alcon Laboratories, Inc., Fort Worth, TX, USA) and FineVision Micro F (PhysIOL SA, Liege, Belgium) in either monocular (P=0.717) or binocular (P=0.837) uncorrected distance vision. Similar results in terms of uncorrected distance vision after implantation of the trifocal lenses AT LISA tri839MP and AcrySof IQ PanOptix and the EDOF lens Tecnis Symfony were also observed in the study by Mencucci et al. (14) Furthermore, in a prospective study of 97 patients conducted by Savini et al. (7), the Mini Well EDOF lens (SIFI, Catania, Italy) was assessed in terms of visual outcome and contrast sensitivity and the investigators reported that the Mini Well EDOF IOL had similar uncorrected distance vision outcomes to previous studies using multifocal IOLs.
The performance of trifocal and EDOF lenses appears to be similar also in the context of intermediate vision. Cochener et al. reported the absence of a statistically significant difference between the two groups of lenses, with a tendency for better outcomes with the EDOF IOL, when emmetropia is the target (3). In the prospective study by Mencucci et al., implantation of the Tecnis Symfony EDOF lens resulted in better outcomes in terms of intermediate vision under mesopic conditions, with a statistically significant difference (P<0.05) being present only when compared to the AT LISA tri839MP IOL and not to the AcrySof IQ PanOptix. However, in photopic conditions, there was no statistically significant difference in uncorrected intermediate vision outcomes between the EDOF and the trifocal IOLs (14). Thus, it seems that the illumination settings may play a crucial role in the performance of each IOL type when intermediate vision is concerned.
Both EDOF and trifocal IOLs achieve spectacle independence for intermediate and distance vision. In terms of near vision, though, trifocal IOLs outperform EDOFs. The latter is clearly depicted in the randomized, comparative study by Cochener et al. (3), which revealed a statistically significant better outcome of both trifocal lenses investigated (AcrySof IQ PanOptix and FineVision Micro F) when compared to the bifocal Tecnis Symfony IOL. This finding is also supported by the studies of Mencucci et al. (14) and Ruiz-Mesa et al. (15) that also point to the superiority of the trifocal IOLs over the EDOF ones for near vision. In fact, Mencucci et al. (14) showed a higher usage of spectacles for near vision in patients who were implanted an EDOF IOL, compared to those who were implanted a trifocal one. Still, the level of post-operative satisfaction was the same for both patient groups (14).
The evaluation of the defocus curve is of great importance as it offers the practitioner and the patient information about the expected visual performance of the IOL over the entire distance spectrum (13). The position of the peaks in the defocus curve is related to the main focal points of the IOLs, hence these curves express the performance and optical imaging of each IOL as a result of its individual design (16). Typically, the bifocal IOLs are associated with a V-shape defocus curve pattern with the highest visual acuity at 0.00 D, resulting in better performance at distance vision, a second peak between ?2.00 and ?2.50 D and a sharp gap for intermediate vision (Figure 1) (7,17).
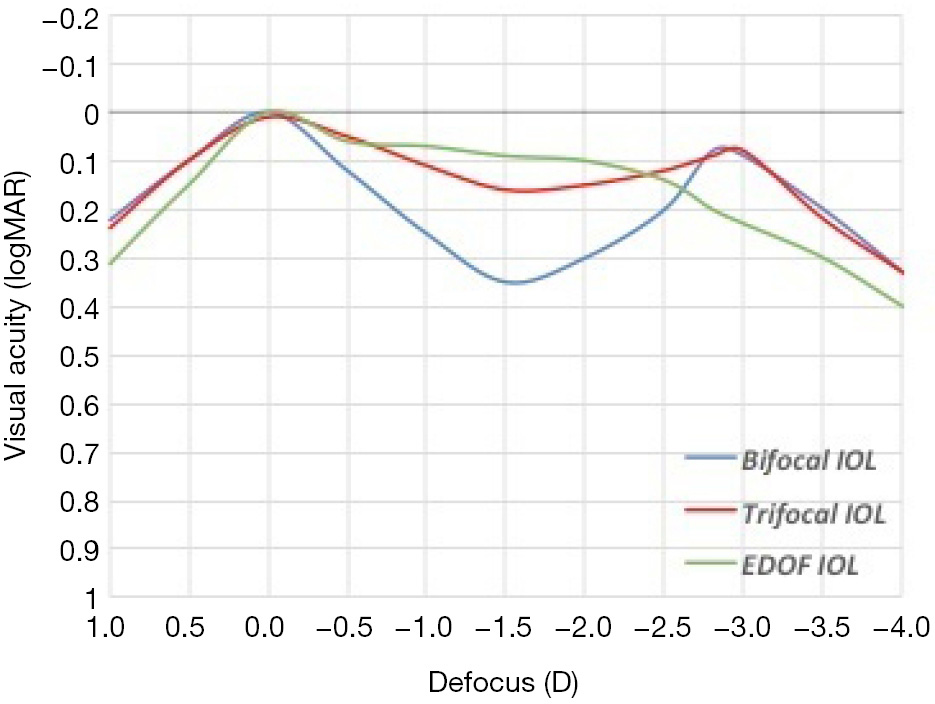
Liu et al. (4) recently compared the visual performance after bilateral implantation of the bifocal IOL AT LISA 809M or the trifocal IOL AT LISA tri 839MP. The defocus curve showed a statistically significant better visual acuity in eyes implanted with trifocal IOLs for defocus of ?1.00 to ?2.00 D (P<0.01), i.e., corresponding to visual distances from 1 m to 50 cm (4). Several additional studies agree with this result (9,18,19) with the meta-analysis of Shen et al. (5) concluding that the trifocal IOLs achieve a better result at defocus of ?1.50 to ?0.50 D and present a significantly better intermediate vision when compared to bifocal IOLs. The superiority of trifocal IOLs for intermediate vision over the bifocal ones comes at no surprise, since the essence of a trifocal IOL is to provide a true intermediate focal point. The comparison of the bifocal and the trifocal defocus curve pattern also demonstrates that, although in some distances bifocal IOLs might have an advantage (9), trifocal IOLs offer a continuum of functional VA at all distances, which in turn translates into higher patient satisfaction relative to bifocal IOLs, since the latter show an abrupt decline of intermediate vision (Figure 1) (5). Interestingly enough, the differences in visual performance between bifocal and trifocal IOLs seem to become more apparent with longer postoperative follow-up (12).
EDOF IOLs produce a smooth, uninterrupted, and dome-shape like defocus curve (3), which provides good quality intermediate vision and tapers off at reading distance (Figure 1) (7). Thus, not surprisingly, EDOF IOLs provide better vision at ?1.00 and ?1.50 D defocus compared to bifocal IOLs (7) and worse near vision than trifocal IOLs at ?2.00 to ?4.00 D defocus (i.e., between 50 and 25 cm) (15).
Finally, it is important to note that multifocal and EDOF IOL performance has also been shown to depend on pupil size. The multifocal and EDOF IOL defocus curves have been analyzed at various pupil diameters, since pupil size may affect everyday tasks such as driving at night or viewing in sunlight. Indeed, for both bifocal and trifocal IOLs, larger pupillary aperture (4.5 mm) was associated with better vision at the 0.00 D focal point (i.e., distance vision), whereas for the rest of the focal points smaller pupil size (3.0 mm) led to better vision (20). EDOF IOLs provided the best vision at 2 mm pupil diameter (11). Trifocal IOLs showcased better pupil independence than both bifocal and EDOF IOLs (11,20,21).
Another aspect highly investigated among the numerous types of IOLs is the post-operative contrast sensitivity they provide, which is regarded as a good surrogate marker of visual function. Cochener et al. (3,22) had argued for the theoretical superiority of EDOF over the trifocal IOLs in terms of contrast sensitivity due to the compensation of chromatic and spherical aberrations by the EDOF IOL design. Mencucci et al. (14) confirmed this hypothesis and demonstrated that the EDOF Tecnis Symfony is associated with enhanced contrast sensitivity, under both photopic and mesopic conditions, when compared to the trifocals AT LISA (0.24 logCS, P<0.001) and IQ PanOptix (0.20 logCS, P<0.001). Ruiz-Mesa et al. (15) did not reach the same conclusion, as they found no statistically significant difference in contrast sensitivity under all illumination settings and spatial frequencies, which may be partially explained by the difference in the contrast sensitivity test utilized in each study. When the comparison involves an EDOF and a bifocal lens, there is absolutely no statistical difference in terms of contrast sensitivity, as stated in the study conducted by Savini et al. (7), which compared the EDOF IOL Mini Well with the bifocal ReSTOR SV25T.
Several methods, such as the Radner and Salzburg reading charts, calculation of the maximum reading speed and the critical print size have been used to assess the effect of the various IOL types on reading ability. One should keep in mind that reading is a complex process that also relies on good attention span and cognitive function. Thus, the results of reading ability assessments should be interpreted with caution.
In the prospective, randomized study by Kaymak et al. (12) the reading performance of patients who underwent implantation of either the trifocal IOL AT LISA tri 839MP or the bifocal IOLs AT LISA 809M and ReSTOR SN6AD1 (Alcon Laboratories, Inc., Fort Worth, TX, USA) was assessed using the Radner reading charts. The reading errors were found to be comparable at 3 and 12 months after surgery between the groups. Moreover, distance corrected maximum reading speed and distance corrected critical print size also exhibited no statistically significant difference between the groups (12).
Kim et al. (23) compared the reading speed for Korean language between two groups of patients who received bilaterally either a trifocal (AT LISA tri 839 MP) or a bifocal (AT LISA 801) IOL of the same material and haptic design. The mean reading speed for font size comparable to a newspaper or a magazine was 86.50±16.34 words per minute (wpm) in the bifocal group and 81.48±27.33 wpm in the trifocal group. Thus, there was no statistically significant difference (P=0.70) between the two groups. In a similar study, Jonker et al. (24) reported a mean reading speed of 145.3±32.9 wpm for the trifocal IOL group and 144.6±38.5 wpm for the bifocal IOL group. This increase in words per minute calculated by Jonker et al. was attributed to the different language (English) involved in the study (23).
Mencucci et al. (14) compared the reading skills of patients who were implanted the trifocal IOLs AT LISA tri 839MP and Acrysof IQ PanOptix and the EDOF Tecnis Symfony IOL under both photopic and mesopic conditions. No statistically significant differences were found in the reading performance among the three different patient groups (P>0.05). The authors speculated that although trifocal lenses exhibited better outcomes for near vision, the enhanced contrast sensitivity of the EDOF lens possibly compensates for the worse near vision with this type of lens, thus leading to similar reading performances (9).
The design of multifocal IOLs is based on the division of light into different foci. Although the addition of new focal points has improved intermediate vision, the focused image is always overlaid by one (bifocal) or two (trifocal) secondary out-of-focus images, coming from the added foci of the IOL (16). Thus, an important aspect of multifocal or EDOF IOL implantation is the occurrence of undesired optical phenomena, which may compromise quality of vision. Optical phenomena include halos, flashes, starbursts, glare and shadows (13). Due to their subjective nature, a quantitative assessment of these phenomena is hard to make. Evaluation of optical phenomena varies across different studies, which makes valid comparisons of different IOLs almost impossible to make (25).
In a study by Alba-Bueno et al. (26) the halos between the Tecnis bifocal IOL with addition powers +4.00, +3.25, and +2.75 D and the trifocal IOLs AT-LISA-tri and FineVision were compared both in vitro and in vivo. The in vitro objective halo assessment in the optical bench revealed that in bifocal IOLs halo size increased with addition power. However, intensity decreased with halo enlargement, possibly due to the larger area available for energy distribution. Furthermore, despite trifocal IOLs creating a halo pattern with two concentric rings, these double halos were less perceived and less annoying for patients than those created by bifocal IOLs (26). Multiple studies have reported no statistically significant difference in the optical phenomena of various multifocal IOLs, with the visual disturbance that patients experience being nonexistent or mild (4,5,25). Halos seem to be more common than glares (4), especially in larger pupillary diameters (i.e., 4.5 mm) (16). The frequency of all the aforementioned phenomena decreases as time goes by, likely due to neural adaptation (4,17).
Comparisons between EDOF and trifocal IOLs showed no difference in the dysphotopic phenomena in the two groups (15). Less than 1% of patients experienced symptoms and of those who did, very few reported disturbances in their everyday life (3,14). Finally, when Savini et al. (7) compared EDOF and bifocal IOLs a few notable differences were found. Halo size and intensity were more prominent in patients with bifocal IOLs while EDOF IOLs seemed to induce fewer night halos.
Over the last 10 years newer IOL technology has revolutionized cataract surgery so that the rising patient expectations of excellent distance, intermediate and near vision can be met. The choice of IOL should depend on each patient’s needs after thorough questioning about their work and daily habits (e.g., use of computers, electronic devices etc.). The main IOL types that have been developed include bifocal, trifocal and EDOF IOLs. In general, trifocal IOLs enhance intermediate vision in comparison to bifocal IOLs, due to the addition of a third focal point, while maintaining good distance and near vision. The EDOF lenses provide better contrast sensitivity and decrease spectacle dependence for distance and intermediate vision, while also being associated with less visual disturbances than bifocal IOLs. However, EDOF lenses are inferior to the trifocal ones in terms of near vision, though this difference does not seem to alter patient satisfaction levels.









