Background: To evaluate efficacy and safety of combined pars plana vitrectomy (PPV) and scleral fixated intraocular lens (SFIOL) surgery as a single procedure.
Methods: Retrospective interventional case series done at a tertiary eye care center in Northern India. Eleven patients who underwent combined PPV and SFIOL surgery were included and analyzed retrospectively.
Results: Mean age of the patients was 43.36±15.12 years (range, 22–64 years). Eight were male. Mean baseline best corrected visual acuity (BCVA) was 0.78±0.63 logMAR units while the mean post-operative BCVA at 6 months follow-up was 0.37±0.29 logMAR units, the visual gain being statistically significant (P=0.021). None of the patients had a drop in BCVA with nine patients having final BCVA better than 0.48 logMAR units. Choroidal detachment (CD) was the only notable complication, seen in three patients. Other complications included two cases of intraoperative retinal breaks, a case each of reversible corneal edema, ocular hypertension and cystoid macular edema.
Conclusions: Combined PPV and SFIOL is an efficacious procedure for managing IOL/lens dislocation and aphakia in a single surgery. There may be short-term reversible complications with no impact on final visual gain.
Combined pars plana vitrectomy (PPV) and scleral fixation of rigid intraocular lens (IOL) has been described previously for closed globe injury sequelae. However, it was often associated with vision threatening complications (1). While micro invasive vitrectomy systems (MIVS) have revolutionized PPV in a major way, scleral fixation of IOL (SFIOL) surgery has also had its share of advancements (2). Lens related complications are a common indication for vitreo-retinal intervention and as current literature supports, both SFIOL and PPV are safe and visually rewarding techniques. Hence, combining the two surgeries as a single step procedure becomes an obvious step towards visual restoration.
In our study we describe the successful management of lens related posterior segment complications with combined PPV and SFIOL using MIVS instruments. We herein discuss the surgical aspects of our technique along with complications encountered during and after surgery.
The study conformed to the tenets of declaration of Helsinki. This was a retrospective analysis of records for 11 patients undergoing combined PPV and SFIOL surgery at a tertiary eye care centre of Northern India. Out of the 11 eyes operated upon, 5 patients had posterior dislocation of lens/lens fragments (3 following complicated cataract surgery, 1 following trauma, 1 in a case of Marfan’s syndrome), 1 had an epi retinal membrane (ERM) and 5 had posterior dislocation of IOL (4 following complicated cataract surgery, 1 following trauma).
All surgeries were performed by a single surgeon (Brijesh Takkar) with the same machine CONSTELLATION? Vision System (Alcon, Fort Worth, Texas, USA) using 25 G instruments. Two patients required intravitreal phacoemulsification and underwent 23 G vitrectomy.
Peribulbar anesthesia was administered to all patients using 5 mL lignocaine hydrochloride 2.0% and 5 mL bupivacaine hydrochloride 0.5%. A superior approach was used for performing the surgery. After a localized peritomy was done at 3 o’clock and 9 o’clock position, the sclera was marked with the help of gentian violet at 1.5 and 3.0 mm from the limbus. Two partial-thickness parallel radial scleral incisions were made between the two marks. A lamellar dissection was then performed between the two incisions with the help of crescent blade to raise a partial-thickness scleral flap (Figure 1A). Bleeding vessels were cauterized and 1 mm tunnels were made perpendicular to the small edge of the rectangle centrally with a 26 G needle (Figure 1B) on both sides, orientation of tunnels aligned to proposed placement of haptics of the IOL.
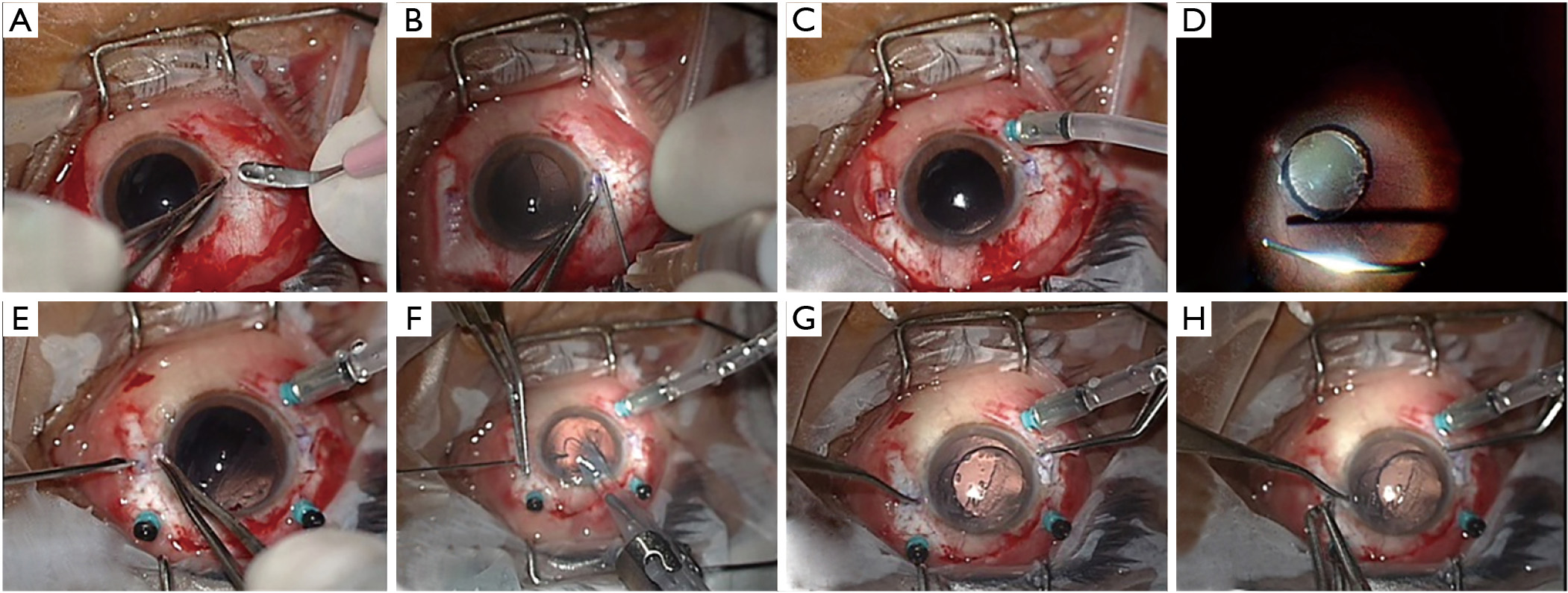
Next conventional 25 G PPV was performed placing the vitrectomy ports away from the scleral flaps (Figure 1C,D). The infusion cannula was placed inferotemporally. For dislocated IOL, the IOL was grasped at the optic-haptic junction with end grasping forceps, and delivered through a limbus based incision. The dropped IOL was repositioned in one case. For dropped lens, phaco fragmentation was performed using linear ultrasound power. Perfluorocarbon liquid was used in all the cases to protect the posterior pole and for easier surgical manipulation. Ports were then plugged for implanting the IOL.
Two sclerotomies were then made with a 23 G microvitreoretinal blade (Alcon, Fort Worth, Texas, USA), one each in the bed of the flap, 1.5 mm from limbus (Figure 1E). A 3.2 mm incision was made at 12 o’ clock with the help of a keratome and a three piece foldable IOL (AcrySof MA60AC, Alcon Laboratories) was introduced into the anterior chamber with the IOL shooter keeping the trailing haptic out of the anterior chamber. The leading haptic of the IOL was guided into the serrated tip of the end gripping 25 G intravitreal forceps and externalized out through the left sclerotomy (Figure 1F). The trailing haptic was then pushed inside the eye with the help of McPherson forceps and similarly externalized out of the eye through the right sclerotomy (Figure 1G). The tips of the haptics were then secured into the dissected scleral tunnel (Figure 1H). Fluid air exchange was done and the retinal periphery was screened in all the cases. Scleral flaps were then sutured. The vitrectomy port sites were sutured only when leaking, else they were left sutureless. The conjunctival flaps were also sutured. Intraoperative and post-operative complications were managed as necessary (Table 1). Figures provided are those from surgery of case 1.
| Case No. | Age (years) | Indication for vitrectomy | BCVA (logMAR) | *Post BCVA (logMAR) | Intraoperative complications | Post-operative complications | Remarks |
|---|---|---|---|---|---|---|---|
| Case 1 | 34 | Post traumatic subluxation of lens | 0.78 | 0.48 | Retinal tear before IOL—laser done and SF6 injected | Corneal edema persistent till 3 weeks | Pigment dispersion with mobile gas bubble |
| Case 2 | 64 | Lens drop | 0.17 | 0.17 | None | CD till 1 week | – |
| Case 3 | 34 | IOL drop | 1.78 | 0.60 | Iris tear during vitrectomy | None | Old macular scar |
| Case 4 | 22 | IOL subluxation | 0.48 | 0.48 | None | CD till 3 days | Old macular scar |
| Case 5 | 56 | Lens drop | 1.18 | 1.00 | None | CD till 3 days | Old corneal opacity |
| Case 6 | 23 | Marfan’s syndrome + post traumatic ACIOL drop | 0.48 | 0.48 | None | None | Intraoperative miosis |
| Case 7 | 59 | IOL drop | 0.48 | 0.30 | Retinal hole with localized retinal detachment after IOL—laser done and SF6 injected | None | – |
| Case 8 | 55 | IOL drop | 0.17 | 0.17 | None | None | IOL repositioned |
| Case 9 | 52 | Lens drop | 1.78 | 0 | None | None | – |
| Case 10 | 48 | Aphakia with dense ERMs | 1.30 | 0.48 | None | Cystoid macular edema till 2 months | IOL haptics placed vertically due to superior anterior synechiae |
| Case 11 | 30 | Marfan’s syndrome with subluxation of lens | 0 | 0 | None | None | Intra operative miosis |
Three pieces foldable IOL (AcrySof MA60AC, Alcon Laboratories) was implanted in all the cases. BCVA, best corrected visual acuity; *Post BCVA, post-operative visual acuity at 3 months of follow-up; IOL, intraocular lens; CD, choroidal detachment; ACIOL, anterior chamber IOL; ERM, epi retinal membrane.
The IOL centration was checked clinically. Intraoperatively, the coaxial light from the microscope was used to form Purkinje images on the cornea and the IOL after re pressurizing the eye. The first primary and the third Purkinje images, from the anterior corneal and anterior surface of IOL respectively, were checked for alignment. This ensured that the IOL was well centred and is a better method than relying on an estimate of the centre of the cornea or of the pupil, both of which may be skewed away from the true visual axis. Post-operatively, pupil was fully dilated and the distance between the posterior surface of iris and the nasal and temporal edges of the optic was noted to identify the tilt of the IOL. Also, the distance between the nasal and temporal edges of the optic and the respective limbus were noted in the fully dilated pupil to identify discrepancy between the two, giving a fair estimate of the amount and the direction of IOL decentration.
All patients had a minimum follow-up of 6 months. They were evaluated after the surgery at day 1, day 7, day 30 and monthly thereafter. At each follow-up, visual acuity, intraocular pressure, centration of IOL and retinal status was evaluated. While collecting the data, emphasis was given to visual results and complications noted during or after the surgery. Macular edema was assessed with spectral domain optical coherence tomography (Cirrus; Zeiss Meditec, Inc., Dublin, CA, USA) at each visit. Statistical analysis was performed using Microsoft excel data sheets and SPSS software (version: 16). Paired t-test was used for analysis of visual acuity in logMAR units.
The mean age of the patients was 43.36±15.12 years (range, 22–64 years). Eight out of 11 patients were male. Mean baseline best corrected visual acuity (BCVA) was 0.78±0.63 logMAR units while the mean post-operative BCVA at 3 months follow-up was 0.37±0.29 logMAR units, the visual gain being statistically significant (P=0.021). None of the patients had a drop in BCVA with nine patients having final BCVA better than 0.48 logMAR units. Details of the patients have been presented in Table 1. The operative time ranged from 75–90 minutes in the 11 patients.
Apart from case 10, all the patients had attained their final BCVA by 1 month of follow-up. The visual acuity remained stable till the six monthly follow-up in all the patients and the mean BCVA was same as at 3 months, 0.37±0.29 logMAR units. In case 10, the gain in visual acuity was slow due to slow resolution of macular edema following removal of a dense ERM (Table 1). The central macular thickness (CMT) was also stable in all the patients apart form case 10. In this patient the pre-operative BCVA was 1.3 logMAR units while the baseline CMT was 420 μm. This patient received topical nepafenac post operatively and had BCVA of 1 logMAR units and CMT of 360 μm at 1 monthly follow-up. By the third monthly follow-up, the BCVA had improved to 0.48 logMAR units while CMT had come down to 290 μm. The patient remained stable thereafter in follow-up.
Only one patient (case 1) had ocular hypertension after surgery, while IOP was within normal limits in all the patients after 1 week of surgery till the final follow-up. The most common complication during surgery was retinal break formation, noted in two patients. In case 1 it occurred at the edge of lattice degeneration during induction of vitreous detachment while in case 7 it was noted after placement of IOL. The most common post-operative complication was choroidal detachment (CD), noted in three patients. Intraoperative miosis was noted in two patients, both established cases of Marfan’s syndrome. Reversible corneal edema and cystoid macular edema were noted in one case each. The IOL was stable in all the patients at final follow-up. IOL haptic breakage or late decentration or IOL tilt were not encountered in any case.
Posterior dislocation of lens and IOL has numerous causes, like iatrogenic, traumatic and spontaneous dislocation, requiring vitrectomy and placement of IOL for visual restoration (1,3). Such situations, often occur in young or middle aged patients, warranting placement of a SFIOL or an anterior chamber IOL (ACIOL). The major long-term complications associated with SFIOL are either retinal (4) or suture related (5,6). Complications are more commonly seen in primary implantation of SFIOL during cataract surgery as compared to secondary rehabilitation (4,7). These findings are partially due to incomplete anterior vitrectomy (6) in primary surgery leading to vitreous traction. Secondary implantation of SFIOL in vitrectomized eyes has been reported to be safe (8). As our technique involves complete vitrectomy, anterior and posterior, along with sutureless IOL fixation, aforementioned complications are not expected to occur. Despite our attempt to complete the vitrectomy, case 7 had a retinal hole with localized retinal detachment noted after placement of the IOL during screening of retinal periphery. It was managed with endolaser and gas injection. As our surgical protocol involved retinal periphery examination after IOL fixation, long term catastrophic effects of such complications were minimized. The ability to thoroughly evaluate the retinal periphery immediately after IOL placement is therefore an advantage of combined PPV and SFIOL approach.
Although we did not encounter dropped IOL while attempting scleral fixation, it could have been easily managed as in case 8 which underwent IOL repositioning (9). This patient had a dropped three pieces foldable IOL following complicated cataract surgery. The surgical technique was same as described above till complete vitrectomy after which perfluoro carbon liquid was injected and the IOL was levitated. The tip of the haptic was gripped with forceps inserted through one of the MVR incisions beneath the scleral flap and externalized and gripped by the assistant. The second haptic was then externalized in a similar fashion. Heavy liquid was removed and the surgery was carried out routinely. Therefore, the ability to reposition and manage “dropped SFIOL” is another major advantage of our technique.
As the surgery is long and can lead to pigment dispersion, we expected ocular hypertension and uveitis in follow-up period (10). However, only one patient, case 1, developed raised IOP (well controlled on medication). This patient had previously documented angle recession with borderline IOP (22 mmHg) in the eye undergoing surgery. Also as gas was injected, the mobile gas bubble could have increased pigment dispersion. This was the only patient in whom corneal edema persisted beyond 3 days. After a month, IOP was well controlled on topical mono therapy with timolol 0.5% and resolution of corneal edema.
The most common post-operative complication noted was CD (11,12). We believe that this is the most important concern with the combined approach. The reason for the same could have been leaking scleral flaps or sclerotomies and inadvertent full thickness scleral perforation during lamellar dissection which went unnoticed. The three patients with CD had slightly low IOP on the first post-operative day (6–10 mmHg) without any evidence of leak on Seidels test. All the three patients received intensive topical steroids and peribulbar steroid injections. In no patient CD persisted beyond 1 week, IOP became normal by the seventh day and no patient required a repeat procedure. This was anticipated pre operatively hence fluid air exchange was done in all the patients. Intraoperative IOP fluctuations can also be the cause and should be controlled.
A previous study on combination of PPV and sutured SFIOL found very high rates of secondary corrective procedures, ~50%, commonly related to haptic breakage (13). Another similar study on 63 eyes found up to 20% late complications, which included two cases of IOL dislocation due to suture breakage (11). A recent study on PPV followed by secondary IOL placement found ERM to occur more commonly after ACIOL placement as compared to sutured SFIOL (14). However the technique of SFIOL has now evolved, with studies showing good results with suture less tucking of the haptics in scleral tunnels (15). In fact if the design of the dropped IOL is suitable, it may be repositioned with or without glue instead of performing an exchange, giving the advantage of lesser surgically induced astigmatism (16,17). In this regard, there have been reports of successful scleral fixation of single piece as well as toric IOLs (18). In our series, however, only one dropped IOL was suitable for repositioning and in others IOL exchange was performed through limbus.
With the combined approach, a need for second surgery is avoided. We did not encounter any IOL decentration. However, there are a few limitations of this technique. First the learning curve is steep. Managing IOP and anterior chamber depth during surgery is particularly challenging. Dependence on a trained assistant to prevent IOL dislocation during attempted scleral fixation is another limitation. Assessment of corneal endothelial cell counts, larger number of patients and longer follow-ups would help in confirming the results and refining the surgery as well. There was no comparative group in our study as it would have become a multiple surgeon study. The technique maybe made completely suture less by avoiding scleral flaps and peritomy all together and placing the haptics of the IOL beneath the conjunctiva (unpublished reports). Large sample sized studies would increase the evidence for the appropriate use of this technique.
Hence combined PPV and SFIOL is an efficacious procedure for managing IOL/lens dislocation and aphakia in a single surgery. While there are no serious long term adverse effects, post-operative short lasting CD is common with no harmful effect on final visual acuity. Other possible complications include intraoperative retinal break, reversible corneal edema and reversible ocular hypertension.