1、Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction(SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes[ J]. Eye Vis (Lond), 2014, 1: 3.Reinstein DZ, Archer TJ, Gobbe M. Small incision lenticule extraction(SMILE) history, fundamentals of a new refractive surgery technique and clinical outcomes[ J]. Eye Vis (Lond), 2014, 1: 3.
2、Boxer Wachler BS, Huynh VN, El-Shiaty AF, et al. Evaluation of corneal functional optical zone after laser in situ keratomileusis[ J]. J Cataract Refract Surg, 2002, 28(6): 948-953.Boxer Wachler BS, Huynh VN, El-Shiaty AF, et al. Evaluation of corneal functional optical zone after laser in situ keratomileusis[ J]. J Cataract Refract Surg, 2002, 28(6): 948-953.
3、Tabernero J, Klyce SD, Sarver EJ, et al. Functional optical zone of the cornea[ J]. Invest Ophthalmol Vis Sci, 2007, 48(3): 1053-1060.Tabernero J, Klyce SD, Sarver EJ, et al. Functional optical zone of the cornea[ J]. Invest Ophthalmol Vis Sci, 2007, 48(3): 1053-1060.
4、Oliveira CM, Ferreira A, Franco S. Wavefront analysis and Zernike polynomial decomposition for evaluation of corneal optical quality[ J].J Cataract Refract Surg, 2012, 38(2): 343-356.Oliveira CM, Ferreira A, Franco S. Wavefront analysis and Zernike polynomial decomposition for evaluation of corneal optical quality[ J].J Cataract Refract Surg, 2012, 38(2): 343-356.
5、Kamiya K, Umeda K, Igarashi A, et al. Factors influencing the changes in coma-like aberrations after myopic laser in situ keratomileusis[ J].Curr Eye Res, 2011, 36(10): 905-909.Kamiya K, Umeda K, Igarashi A, et al. Factors influencing the changes in coma-like aberrations after myopic laser in situ keratomileusis[ J].Curr Eye Res, 2011, 36(10): 905-909.
6、Jin HY, Wan T, Wu F, et al. Comparison of visual results and higher-order aberrations after small incision lenticule extraction (SMILE): high myopia vs. mild to moderate myopia[J]. BMC Ophthalmol, 2017, 17(1): 118.Jin HY, Wan T, Wu F, et al. Comparison of visual results and higher-order aberrations after small incision lenticule extraction (SMILE): high myopia vs. mild to moderate myopia[J]. BMC Ophthalmol, 2017, 17(1): 118.
7、Racine L, Wang L, Koch DD. Size of corneal topographic effective optical zone: comparison of standard and customized myopic laser in situ keratomileusis[ J]. Am J Ophthalmol, 2006, 142(2): 227-232.Racine L, Wang L, Koch DD. Size of corneal topographic effective optical zone: comparison of standard and customized myopic laser in situ keratomileusis[ J]. Am J Ophthalmol, 2006, 142(2): 227-232.
8、Chan TCY, Wan KH, Kang DSY, et al. Effect of corneal curvature on optical zone decentration and its impact on astigmatism and higher-order aberrations in SMILE and LASIK[ J]. Graefes Arch Clin Exp Ophthalmol, 2019, 257(1): 233-240.Chan TCY, Wan KH, Kang DSY, et al. Effect of corneal curvature on optical zone decentration and its impact on astigmatism and higher-order aberrations in SMILE and LASIK[ J]. Graefes Arch Clin Exp Ophthalmol, 2019, 257(1): 233-240.
9、Camellin M, Arba Mosquera S. Aspheric optical zones: the effective optical zone with the SCHWIND AMARIS[ J]. J Refract Surg, 2011,27(2): 135-146.Camellin M, Arba Mosquera S. Aspheric optical zones: the effective optical zone with the SCHWIND AMARIS[ J]. J Refract Surg, 2011,27(2): 135-146.
10、Hou J, Wang Y, Lei Y, et al. Comparison of effective optical zone after small-incision lenticule extraction and femtosecond laser-assisted laser in situ keratomileusis for myopia[ J]. J Cataract Refract Surg, 2018,44(10): 1179-1185.Hou J, Wang Y, Lei Y, et al. Comparison of effective optical zone after small-incision lenticule extraction and femtosecond laser-assisted laser in situ keratomileusis for myopia[ J]. J Cataract Refract Surg, 2018,44(10): 1179-1185.
11、Qian Y, Huang J, Zhou X, et al. Corneal power distribution and functional optical zone following small incision lenticule extraction for myopia[ J]. J Refract Surg, 2015, 31(8): 532-538.Qian Y, Huang J, Zhou X, et al. Corneal power distribution and functional optical zone following small incision lenticule extraction for myopia[ J]. J Refract Surg, 2015, 31(8): 532-538.
12、Fu D, Wang L, Zhou X, et al. Functional optical zone after small-incision lenticule extraction as stratified by attempted correction and optical zone[ J]. Cornea, 2018, 37(9): 1110-1117.Fu D, Wang L, Zhou X, et al. Functional optical zone after small-incision lenticule extraction as stratified by attempted correction and optical zone[ J]. Cornea, 2018, 37(9): 1110-1117.
13、Dong Z, Zhou X, Wu J, et al. Small incision lenticule extraction(SMILE) and femtosecond laser LASIK: comparison of corneal wound healing and inflammation[ J]. Br J Ophthalmol, 2014, 98(2): 263-269.Dong Z, Zhou X, Wu J, et al. Small incision lenticule extraction(SMILE) and femtosecond laser LASIK: comparison of corneal wound healing and inflammation[ J]. Br J Ophthalmol, 2014, 98(2): 263-269.
14、Mohamed-Noriega K, Riau AK, Lwin NC, et al. Early corneal nerve damage and recovery following small incision lenticule extraction(SMILE) and laser in situ keratomileusis (LASIK)[ J]. Invest Ophthalmol Vis Sci, 2014, 55(3): 1823-1834.Mohamed-Noriega K, Riau AK, Lwin NC, et al. Early corneal nerve damage and recovery following small incision lenticule extraction(SMILE) and laser in situ keratomileusis (LASIK)[ J]. Invest Ophthalmol Vis Sci, 2014, 55(3): 1823-1834.
15、Yu M, Chen M, Liu W, et al. Comparative study of wave-front aberration and corneal Asphericity after SMILE and LASEK for myopia: a short and long term study[ J]. BMC Ophthalmol, 2019, 19(1): 80.Yu M, Chen M, Liu W, et al. Comparative study of wave-front aberration and corneal Asphericity after SMILE and LASEK for myopia: a short and long term study[ J]. BMC Ophthalmol, 2019, 19(1): 80.
16、Ang M, Tan D, Mehta JS. Small incision lenticule extraction (SMILE) versus laser in-situ keratomileusis (LASIK): study protocol for a randomized, non-inferiority trial[ J]. Trials, 2012, 13: 75.Ang M, Tan D, Mehta JS. Small incision lenticule extraction (SMILE) versus laser in-situ keratomileusis (LASIK): study protocol for a randomized, non-inferiority trial[ J]. Trials, 2012, 13: 75.
17、Gyldenkerne A, Ivarsen A, Hjortdal J?. Comparison of corneal shape changes and aberrations induced by FS-LASIK and SMILE for myopia[ J]. J Refract Surg, 2015, 31(4): 223-229.Gyldenkerne A, Ivarsen A, Hjortdal J?. Comparison of corneal shape changes and aberrations induced by FS-LASIK and SMILE for myopia[ J]. J Refract Surg, 2015, 31(4): 223-229.
18、赵艳, 孙西宇, 王晓睿, 等. FS-LASIK两种光学区直径术后视觉质量的比较[ J]. 国际眼科杂, 2019, 19(8): 1373-1376.
ZHAO Yan, SUN Xining, WANG Xiaorui, et al. Comparison of two optical zones in visual quality after femtosecond laser-assisted Lasik[ J].International Eye Science, 2019, 19(8): 1373-1376.赵艳, 孙西宇, 王晓睿, 等. FS-LASIK两种光学区直径术后视觉质量的比较[ J]. 国际眼科杂, 2019, 19(8): 1373-1376.
ZHAO Yan, SUN Xining, WANG Xiaorui, et al. Comparison of two optical zones in visual quality after femtosecond laser-assisted Lasik[ J].International Eye Science, 2019, 19(8): 1373-1376.
19、Seo KY, Lee JB, Kang JJ, et al. Comparison of higher-order aberrations after LASEK with a 6.0 mm ablation zone and a 6.5 mm ablation zone with blend zone[ J]. J Cataract Refract Surg, 2004, 30(3): 653-657.Seo KY, Lee JB, Kang JJ, et al. Comparison of higher-order aberrations after LASEK with a 6.0 mm ablation zone and a 6.5 mm ablation zone with blend zone[ J]. J Cataract Refract Surg, 2004, 30(3): 653-657.
20、陈弯, 李莉, 刘胜旭, 等. SMILE与FS-LASIK术后光学区特性比较[ J]. 中华眼视光学与视觉科学杂志, 2020, 22(5): 333-340.
CHEN Wan, LI Li, LIU Shengxu, et al. Comparison of the actual optical zones after SMILE and FS-LASIK for myopia[ J]. Chinese Journal of Optometry Ophthalmology and Visual Science, 2020, 22(5):333-340.陈弯, 李莉, 刘胜旭, 等. SMILE与FS-LASIK术后光学区特性比较[ J]. 中华眼视光学与视觉科学杂志, 2020, 22(5): 333-340.
CHEN Wan, LI Li, LIU Shengxu, et al. Comparison of the actual optical zones after SMILE and FS-LASIK for myopia[ J]. Chinese Journal of Optometry Ophthalmology and Visual Science, 2020, 22(5):333-340.
21、Wu W, Wang Y. Corneal higher-order aberrations of the anterior surface, posterior surface, and total cornea after SMILE, FS-LASIK,and FLEx surgeries[ J]. Eye Contact Lens, 2016, 42(6): 358-365.Wu W, Wang Y. Corneal higher-order aberrations of the anterior surface, posterior surface, and total cornea after SMILE, FS-LASIK,and FLEx surgeries[ J]. Eye Contact Lens, 2016, 42(6): 358-365.
22、Waheed S, Chalita MR, Xu M, et al. Flap-induced and laser-induced ocular aberrations in a two-step LASIK procedure[ J]. J Refract Surg,2005, 21(4): 346-352.Waheed S, Chalita MR, Xu M, et al. Flap-induced and laser-induced ocular aberrations in a two-step LASIK procedure[ J]. J Refract Surg,2005, 21(4): 346-352.
23、Wu D, Wang Y, Zhang L, et al. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis[ J]. J Cataract Refract Surg, 2014, 40(6): 954-962.Wu D, Wang Y, Zhang L, et al. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis[ J]. J Cataract Refract Surg, 2014, 40(6): 954-962.

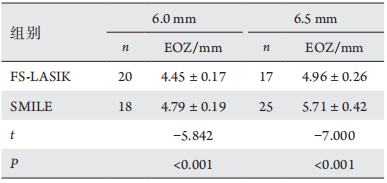
 EOZ直径为6条主子午线EOZ直径的平均值,记为EOZ。
EOZ直径为6条主子午线EOZ直径的平均值,记为EOZ。