Abstract: The article discusses the early abandonment of mechanical theories about eye enlargement in degenerative myopia at the turn of the 20th century. At that time, the number of theories about myopia grew unrestricted, but with scant support from the experimental field. The mechanical theories vanished as a new wave of metabolism-based theories appeared, propelled by the huge advances in molecular biology. Modern techniques allow reconsidering those theories and to put them to test with higher confidence.
The article discusses the early abandonment of mechanical theories about eye enlargement in degenerative myopia at the turn of the 20th century. At that time, the number of theories about myopia grew unrestricted, but with scant support from the experimental field. The mechanical theories vanished as a new wave of metabolism-based theories appeared, propelled by the huge advances in molecular biology. Modern techniques allow reconsidering those theories and to put them to test with higher confidence.
Myopia is a complex phenomenon in which both genes and environment play a still indeterminate role. Arguably, myopia depends on genetic and environmental factors. Myopia is mainly inherited in a polygenic fashion. Monogenic inheritance is a rarity. Most studies put emphasis on a discrete value of spherical refraction (?5.0 or ?6.0 D) (1) to delimit mild from pathologic myopia, but the fact is that there is an almost direct, but not complete, relationship between axial length and chorioretinal degeneration and that limits based on spherical values are artificial. The number of epidemiological studies based on axial length is scant.
The problem posed by degenerative myopia cannot be overstressed. Degenerative myopia is one of the leading causes of world blindness. Reportedly, 5 billion people will be diagnosed with myopia by 2050, among them, 1 billion at risk for going blind. Myopia has become prevalent in East Asia, where up to 90 percent of school children in the urban areas have some degree of vision loss. The problem is growing in Western nations as well (2).
The main changes associated with the thinning of the sclera, accompanied occasionally with lacquer cracks and staphylomas, are atrophy of the retinal pigment epithelium (RPE) and choroid that start in the choriocapillaris and retinal thinning. Choroidal changes frequently lead to the proliferation of RPE, neovascularization, and hemorrhages (3).
But what can we do to help? There are few resources to arrest the degenerative process and no way to recover lost vision. Apart from the traditional ways of refractive correction, our arsenal is reduced to a few hygienic counsels: “Parents should encourage their children to spend time outdoors for at least two hours each day” (4).
There is a relative consensus that the mechanism of retinal degeneration is related to choroidal rarefaction, linked to ocular enlargement. However, although there is an admitted relationship between visual habits and myopia, the intimate mechanisms that cause ocular enlargement are not precisely known. Two main theoretical grounds stand up: the biomechanical and the heredodegenerative. Classically, the mechanical theory has pointed to the role of extraocular muscles (EOMs) and intraocular pressure (IOP) as causative factors.
Duke-Elder [1970] (5), classifies the attitudes about myopia in two opposing sides: a classical conception held that the degenerative changes in the myopic eye were secondary to distension of the coats of the eyeball mainly due to influences of the environment and determined by the health and the habits of the patient.
The main defenders of the classical theory of scleral distension were Von Graefe [1857], which supported the role of IOP on eye enlargement. Another proponent of the raised IOP was Dobrowolski [1868] who pointed to the action of the intrinsic muscles during accommodation. Stilling [1985–1905] speculated with a tractional role of the superior oblique (SO) and though of myopia as a peculiar form of glaucoma. Another early muscle adherent was Manhart [1871], who attributed a role to the overaction of the recti muscles. The mechanical distension of the external coat of the eye was allegedly assisted by a weakened sclera of diverse origin.
Wholly opposed to this line of thought, the biological theories led by Steiger [1913] but popularized by Vogt [1924] and his disciples insisted in a predominance of hereditary factors. In short, they assumed that each ocular coat has a growth potential, being the retina the master tissue. Harmonized development of the three coats gives rise to an emmetropic eye, and an overgrow of the retina results in myopia.
The relative importance of the environment and heredity on the development of myopia has varied in the medical records since then, and the same Duke-Elder favored the biological side. The current spectacular development of molecular biology has increased the research activity in the metabolic activity of the retina.
The heredodegenerative theory contemplates an abiotrophic retinal process independent of the changes of the scleral coat (6). In spite of intensive search, the biochemical path leading to myopia is far from clear. An increasing number of biomarker is being identified, but the list is long and inconclusive. Increased levels of hyaluronidase, cortisol, somatotropic hormone or alkaline phosphatase have been found in the blood of myopic patients. Furthermore, the fall of copper concentration in the sclera and the increase of free radicals in the vitreous have been reported. However, many other molecules appear as significant, among other high levels of aspartate, threonine, serine, glutamate and others.
Recent research has continued and expanded the search of mechanical processes such as accommodation, light focus, light incidence, light color, IOP, and others (4), but mechanical action by the EOMs is conspicuously absent.
Previously, a common trend was to separate the process of emmetropization and myopization. However, current studies in experimental myopia have corrected this tendency. Experimental myopia assumes a relationship between emmetropization and myopization; both share the same mechanisms with a variation in timing (7).
Apart from monkeys, all animal models studied up to date show important divergences from human and, consequently, must be interpreted with caution (Morgan 2014). Currently, most, if not all, experimental models of myopia, deal with biomolecular mechanisms to try to explain retinal, choroidal and scleral degenerative processes. Several animal models are being developed, including recently introduced knock-out mouse models, lacking some of the presumed elements of the signalling cascade involved in the metabolic machinery responsible for the enlargement of the sclera (8).
Because of the incipient surgical techniques at the time, the question of EOM involvement in myopia was prematurely abandoned in the early 20th century. As a result, the participation of the extra and intraocular muscles in scleral distension has not been appropriately dealt with. Nowadays, we have the technology to rule out (or confirm) definitively the involvement of mechanical forces acting on the outside as well as in the inside of the eye, via extrinsic and intrinsic ocular muscles. A set of appropriate, well-designed experiments should be performed to avoid a false closure.
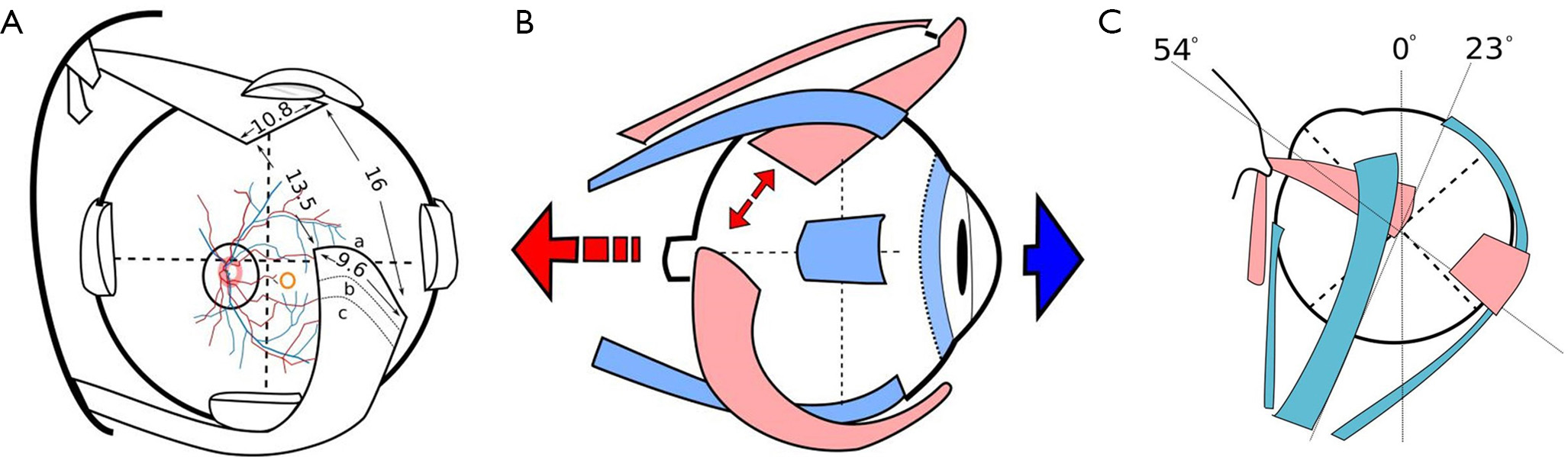
The EOMs are able to contract with fiber shortening (isotonic contraction) or without fiber shortening (isometric contraction). By a combination of both types of contraction, the eye rotates around two areas known as space and body centrodes, situated 13.5 mm behind the cornea and nasally displaced from the geometrical center of the globe (9). To accomplish the formidable task of accessing virtually infinite positions, the EOMs are endowed with unusual physiological characteristics that derive from their expression of specific contractile proteins including, myosin heavy chain isoforms, myosin light chains, tropomyosin, and troponin, connected in parallel or in series, and other special features. The EOM myofiber continuum hypothesis combined with the non-linearity of eye muscle contractile properties would explain a total central nervous system (CNS) control of muscle tone and eye position and velocity. In EOM there seems to be a continuum of myofiber types. Each myosin heavy and light chain isoform results in a distinct shortening velocity, which would translate in an increased plasticity in the control of muscle force generation (10).
It can be argued that an anterior group of recti muscles acting jointly with isometrical contraction would fix the eye, while the ciliary muscle would pull anteriorly the choroid. At the same time, the joint action of both oblique muscles, acting isotonically, would pull apart the posterior pole, with the result of eye enlargement. The angle formed by the obliques and the ocular axis ranges in the low fifties [51° for inferior oblique (IO) and 54° for SO]. Convergence is the position of the globe in which the elevator and depressor action of the obliques is maximal. This is the near (reading) position with a synergy with accommodation (and miosis). In this position, the four recti can maintain the globe fixed with a tonic grip, while the maximal conjunct action of the obliques pulls the posterior pole apart, causing the elongation of the globe in its post-equatorial half (Figure 1). Scleral pulling would secondarily cause choroidal stretching and rarefaction.
A recent study relates severe IO overaction to thinning of the subfoveal choroid, attributable to external mechanical effect (13). Myopia and near-work are statistically related in many studies, although also here are appearing divergent results (14,15).
Fortunately, this theory can be disproved (or confirmed) in an experimental setting in which the experimentally induced myopia can be totally neutralized, as regard to the muscular action, by the use of botulinum toxin (BT) injected into the EOMs. BT should be tested with and without cycloplegic drops, to paralyze accommodation. The effectivity of the induced muscle paralysis can be monitored, in the experimental animal, with electromyography.
Purified BT, produced by the anaerobic bacterium Clostridium botulinum, specifically targets the release of acetylcholine. Out of seven distinct antigenic BTs (A to G) produced by different strains of Clostridium botulinum, the human nervous system responds to five toxin serotypes but is unaffected by serotypes C and D. Each species has its own response. Currently, only the A and B toxins are available as drugs. BT irreversibly binds to the presynaptic terminal of the neuromuscular junction, where it cleaves membrane proteins responsible for acetylcholine excretion. In the design of the experiment, it is essential to take into account that the peak action of the BT does not occur immediately, and its maximum effect may take up to a couple of weeks. Additionally, BT’s action slowly decreases over time (16).
To my knowledge, this experiment has not yet been done. However, it could definitively incline the balance towards either side. The importance of answering to the role played in myopization by the extra and intraocular muscles cannot be overemphasized as it could lead to new therapeutic modalities.









