Objectives: To evaluate the performance of orthokeratology (ortho-k) lens reordering using software-designed system, so as to determine the feasibility of ortho-k lens reordering without discontinuing lens wear. Methods: This study is a retrospective analysis of data of ortho-k lens wearers who had a history of short-term discontinuation of lens wear. A total of 94 individuals aged over 8 years with spherical equivalent refraction ranging from -0.50 to -6.50 diopters were included. The corneal topography data at baseline (before ortho-k) and after lens wear discontinuation (cessation of ortho-k treatment) were imported separately into the lens-design software, along with corresponding refraction data. Subsequently, corneal and lens parameters were generated and compared. Intraclass correlation coefficients (ICC) were calculated, and Bland and Altman analyses were conducted. Results: All 94 children were involved in the retrospective analysis. Compared with baseline data, there was a high level of consistency between Rwo (without discontinuation) and Rwith (with discontinuation), with an ICC of 0.96 (P<0.001). Furthermore, the comparison of lens parameters generated by the Easyfit software between baseline and after short-term discontinuation showed a high degree of consistency, with all of the ICC values exceeding 0.90. Similar results were obtained using the WAVE software, as both ICC values and Bland-Altman plots demonstrated a high level of consistency in lens parameters between two conditions (nearly all data points fell within the 95% LoAs ). Conclusions: It is feasible to directly reorder new ortho-k lenses using software fitting approaches. However, further investigations are ncessary to validate their practicability in a clinical setting.
Objectives: To evaluate the performance of orthokeratology (ortho-k) lens reordering using software-designed system, so as to determine the feasibility of ortho-k lens reordering without discontinuing lens wear. Methods: This study is a retrospective analysis of data of ortho-k lens wearers who had a history of short-term discontinuation of lens wear. A total of 94 individuals aged over 8 years with spherical equivalent refraction ranging from -0.50 to -6.50 diopters were included. The corneal topography data at baseline (before ortho-k) and after lens wear discontinuation (cessation of ortho-k treatment) were imported separately into the lens-design software, along with corresponding refraction data. Subsequently, corneal and lens parameters were generated and compared. Intraclass correlation coefficients (ICC) were calculated, and Bland and Altman analyses were conducted. Results: All 94 children were involved in the retrospective analysis. Compared with baseline data, there was a high level of consistency between Rwo (without discontinuation) and Rwith (with discontinuation), with an ICC of 0.96 (P<0.001). Furthermore, the comparison of lens parameters generated by the Easyfit software between baseline and after short-term discontinuation showed a high degree of consistency, with all of the ICC values exceeding 0.90. Similar results were obtained using the WAVE software, as both ICC values and Bland-Altman plots demonstrated a high level of consistency in lens parameters between two conditions (nearly all data points fell within the 95% LoAs ). Conclusions: It is feasible to directly reorder new ortho-k lenses using software fitting approaches. However, further investigations are ncessary to validate their practicability in a clinical setting.
HIGHLIGHTS
· Advances in orthokeratology lens fitting technology now enable a software-based fitting system to seamlessly reorder new lenses using baseline corneal topography data, thereby eliminating the need for short-term discontinuation of lens wear.
· The study employed a retrospective study design of 94 ortho-k wearers evaluating corneal changes after short-term lens discontinuation. Comparing corneal and lens parameters generated from pre-treatment and post-cessation data. Additionally, assessed agreement using Intraclass Correlation Coefficients (ICC) and Bland-Altman analysis.
· Insights from the current study may enhance our comprehension of the software-assisted lens design system, offering significant time savings and more convenience for lens wearers. In the future, the feasibility of using baseline topography to directly reorder new lenses for required wearers needs to be clinically validated.
INTRODUCTION
In recent decades, myopia has reached epidemic proportions among young people in East and Southeast Asia, especially in China. This underscores the importance of recognizing the necessity of refractive correction due to the increased risk of myopic-related complications, such as retinal detachments,[1, 2] maculopathies,[3] and choroidal neovascularization.[4]Numerous studies have demonstrated the myopia control effect of orthokeratology (ortho-k), which has garnered increasing attention and widespread clinical use in China.[5-8]
However, ortho-k lens must be worn for extended periods to suppress axial length elongation.[6] Typically, a large group of long-term wearers require lens reordering for various reasons, including loss of lens, prescription updates due to myopia progression, or routine checkup (usually every 3 or 6 months, as recommended by optometrists) without pior complaints.[9, 10] Notably, these patients are often instructed to discontinue lens wear for at least one month, after which optometrists reorder new lenses based on new baseline corneal topography and refraction measurement obtained following lens cessation (Rwith), performed by an examiner.[11] This one-month or longer waiting period not only wastes time but also disrupts patients’ studies, daily life and even visual experience.[12] As the "lens reorder" phenomenon becomes increasingly common in clinic practice, the prolong waiting time for cornea recovery represents a major challenges, imposing significant inconvenience on lens wearers.[13, 14] In other words, for long-term ortho-k lens wearers, little is known about whether it reasonable to reorder new lenses based on baseline corneal topography and simulated refraction after long-term wear without discontinuing lens use (Rwo), as predicted by an experienced formula using baseline data.
Therefore, a reordering procedure that eliminates the need for short-term lens wear discontinuation is warranted to save time for both patients and optometrists. Fortunately, software-based order system,which enable direct lens ordering based on cornal topography without trial lens fitting, have been shown to be time-efficient and clinically effective.[13, 15-19] However, these systems still inevitably face the issue of lens wear discontinuation for ortho-k reordering. To date, successful reordering cases without short-term discontinuation have primarily relied on optometrist’s clinical experiences.[20] Only a few studies have reported the impact of topographic changes on reordered lens parameters and recommended adjustments.[9, 18] Similarly, with the growing popularity of lens fitting software, it is worth exploring whether such software-based system can directly reorder new lenses using baseline corneal topography without requiring lens wear discontinuation.
In this study, two software-based lens ordering systems were used to assist in three-curve Menicon Z Night (NKL Contactlenzen, Netherlands) and four-zone WAVE (SDJ MasterVision Corporation, Tianjin, China), respectively. The objective of this study is to evaluate the feasibility of using a software-based system to directly reorder new lenses using baseline corneal topography without lens wear discontinuation . If feasible, this approach would not only enhance convenience for lens wearers but also provide clinical guidance for future ortho-k lens design, holding significant clinical implications.
METHODS
Participants
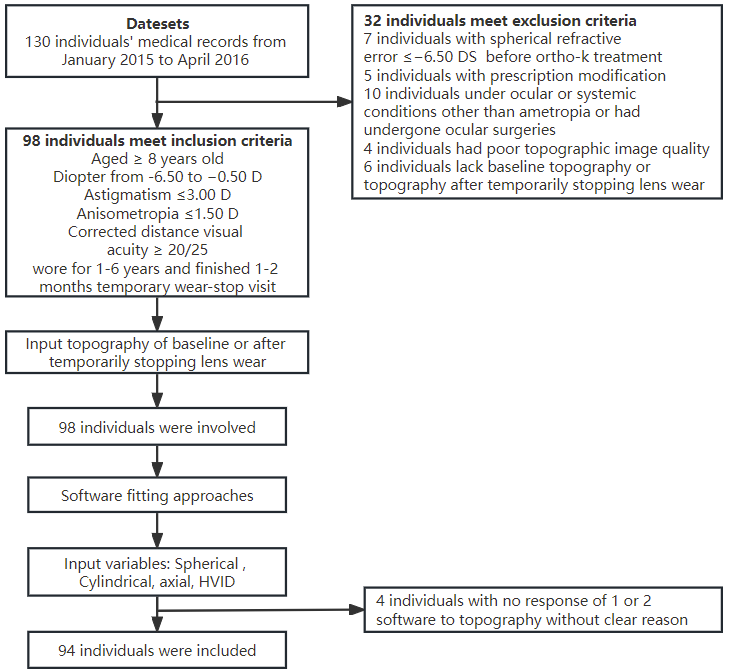
This retrospective study adhered to the tenets of the Declaration of Helsinki, and ethical approval was obtained from the Institutional Review Board/Ethics Committee of Sun Yat-sen University (Guangzhou, China) for this retrospective analysis. This study analyzed data collected from 94 eyes of 94 Chinese individuals aged over 8 years with myopia who were fitted with five types of ortho-k lenses for myopia management at the Zhongshan Ophthalmic Center between January 2015 and April 2016. Patient identification was based on corneal topography and relative demographic information. The five ortho-k brands used in this study cover two lens designs that currently dominate the international market. Specifically, Menicon Z Night (NKL Contactlenzen, Netherlands) and Paragon corneal refractive therapy (CRT) (Paragon CRT, Paragon, Gilbert, AZ, United States) both featured a three-curve design. The other three brands, Emerald Series (Euclid, USA), WAVE (SDJ MasterVision Corporation, Tianjin, China) and Alpha ORTHOK (Alpha Orthokeratology, Alpha Corporation, Nagoya, Japan), are all designed based on the Vision Shaping Treatment (VST) lens model, which incorporates a four-zone reverse geometry design. Inclusion criteria were as follows: subjects with cycloplegic spherical power ranging from −6.50 to −0.50 diopters (D), astigmatism≤ 3.00 D, and corrected distance visual acuity equal to or better than 20/25 or better. The subjects were aged between 8 and 45 years (11.9 ± 4.9). Only individuals who had been undergoing ortho-k therapy for 1 to 6 years (37.4 ± 11.9 months) at the time of enrollment were included. These patients were required to discontinue lens wear for various reasons, including prescription updates due to myopia progression, routine checkups prior to reordering, or loss of lens (Figure 1). In all cases, the lens wear discontinuation period was 1-2 months, reflecting the most common clinical scenario. Exclusion criteria were as follows: 1) pre-ortho-k spherical refractive error greater than −6.50 DS based on noncycloplegic manifest refraction; 2) ocular or systemic conditions other than ametropia, or a history of ocular surgeries; 3) poor-quality topographic measurement that could not be recognized by software; 4) lack of topographic images at baseline or after lens wear discontinuation(Figure 1). The final lens parameters, confirmed by both fluorescein staining at lens delivery and an ideal "bull’s-eye" corneal topography pattern after ortho-k treatment, were prescribed by the same doctor. No severe corneal complications were observed during follow- up. Mild corneal staining without self-reported symptoms was the most common side effect; however, due to the lack of recorded symptom data, the incidence of lens-related ocular surface response, such as corneal staining, could not be calculated. Among these patients, 35 were male and 59 were female, with a mean age of 11.9 ± 4.9 years( range from 8 to 45 years). To eliminate interocular correlation effects, only data from the right eyes were included in this study.
Research framework and data processing
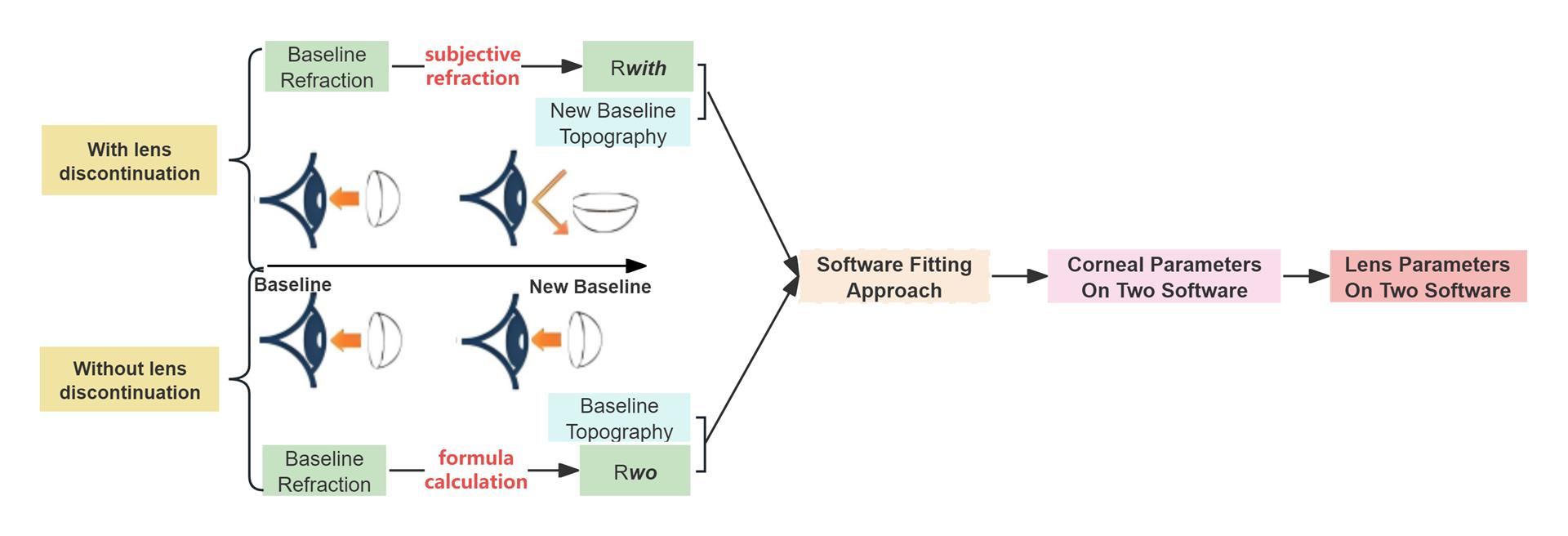
The general research procedure. The research framework and data processing workflow of this study is illustrated in Figure 2. Previously, in a randomized controlled trial , a software-based lens ordering system, was proposed to determine ortho-k lens parameters using corneal elevation data.[15] This approach demonstrated superior clinical performance compared to traditional fitting trial. In the present study, we employed two software-based systems: Easyfit software( for NKL lenses, a three-curve-designed lens similar to CRT) and the WAVE contact lens system(for WAVE lens , featuring a four-zone reverse geometry design). After importing corneal topography data into the computers equiped with these software packages, corneal profile information was automatically recognized and extracted. Subsequently, refraction data and HVID were input into the software, generating lens type specifications, a series of lens parameters, and even fitting simulation figures. Due to differences in operating principles and application scope between the two software systems, the lens parameters they generated also varied. The lens design order interface is shown in Supplemental Figure 1. To compare differences in software-generated lens and corneal parameters between baseline and post-lens wear discontinuation, we first imported the baseline topography data with Rwo. After short-term discontinuation, we re-imported updated topography with Rwith , enabling the generation of corresponding parameters under each condition.
Two Approaches: by simulating the Condition of lens reorder with or without short-term lens wear discontinuation. The primary procedure difference between using baseline versus post-discontinuation topography lies in the refractive data input. For baseline topography, Rwo must be predicted under the assumption of "reordering a new lens without lens wear discontinuation". In contrast, for post-discontinuation topography, Rwith is directly input into the software to facilitate lens reordering. To address this, we utilized an empirically validated formula, based on axial elongation over time, to calculate Rwo This formula has been integrated into our clinical protocols for several years, demonstrating high accuracy and reliability[17]. The refractive formula accounts for both physiological and myopic-related axial elongation, with 0.1 mm of elongation corresponding to an additional 0.25 D of myopia progression beyond emmetropia, supported by clinical evidence and extensive literature.[17] By simulating scenarios of lens reordering with or without lens wear discontinuation, we compared and analyzed the consistency of software-generated lens parameters derived from baseline versus post-discontinuation topography. The refractive formula was calculated based on the principle that 1 millimeter of axial elongation corresponds to 2.50 diopter of myopia progression.[21, 22] Here, Visit AL refers to the axial length (in mm) measured at the last visit before lens reordering, Baseline AL denotes the axial length at baseline ( prior to ort
ho-k treatment),and Physiological △AL represents the expected axial elongation due to normal eye growth in myopic children from ages 6 to 15 years.[23, 24]
Lens parameters generated on two software
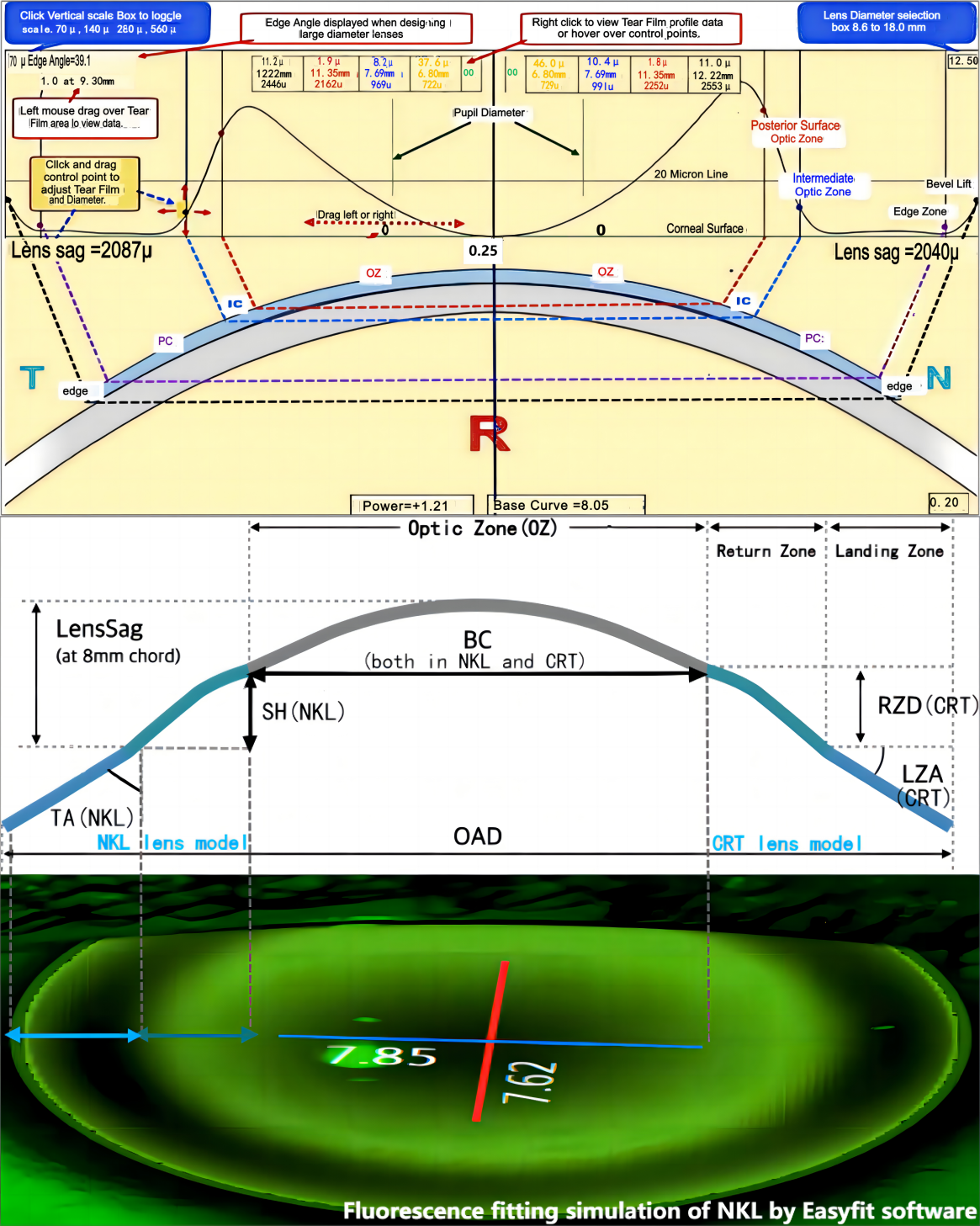
As mentioned in the previous sections, the Easyfit software(produced by Menicon company) was originally developed for designing Menicon Z Night lens (NKL). Due to its similar lens design principles to CRT lenses, both feature a Base Curve (BC) that applies pressure to cornea. However, the Return Zone Depth (RZD) in the CRT model corresponds to the sagittal Height (SH) in NKL, with the primary difference being the Tangential angle (TA) in NKL versus the Landing Zone Angle (LZA) in CRT lenses. Consequently, the Easyfit software is also suitable for CRT and CRT-like designs. The lens parameters generated by the Easyfit software consists of four main components. First, the lens type is determined, which is critical for deciding whether a toric design is required. Subsequently, the remaining parameters, BC, Horizontal SH, Horizontal TA, are generated. If a toric design is necessary, two more parameters, Vertical SH and Vertical TA are also generated, are also identical to those in CRT toric lenses (Supplemental Figure 1).
In contrast, the WAVE contact lens system,introduced from America several years ago, enables lens ordering without diagnostic fitting [18] and has gained popularity in China due to its high first-fit success rate. Notably, as it is compatible with lens based on VST model( which captures the entire Chinese market), the WAVE software can design lenses for multiple brands, including Euclid, Lucid and Alpha.[22] A summary of WAVE lens design parameters includes: Lens Geometry, BC, OAD, CT, ET, JF. To control variables, OAD, CT, ET and JF were designed to match those of NK lens under Geometric Symmetric mode. As shown in Supplemental Figure 1, the WAVE interface generates numerous lens-related indices beyond BC, including Lens sagittal depth (SAG) at four positions (OZ, IC, PC and edge) along eight semi-meridians (0°, 45°, 90°, 135°, 180°, 225°, 270° and 315°). By holding the left mouse button down and dragging the cursor, users can view data such as Tear Layer, Lens Sag, and Distance from center in the Lens Profile Window. For example, "horizontal Lens SAG at IC" refers to the sagittal depth at the IC position along the horizontal meridian.Selecting a new semi-meridian in the simulated fluorescein view updates the Lens Profile and Tear Film Graph will change accordingly.To minimize variability and reduce bias, the following parameters were kept consistent with NKL: Jessen Factor equals to 1, BOZD is 6 mm, and lens thickness is 0.22 mm. Considering these factors, we primarily compared the consistency of BC, SAG of lens at OZ, IC, PC and edge along horizontal and vertical meridians (0°, 90°, 180°, 270°) between baseline and post-lens wear discontinuation. Although Tear Layer Thickness (TLT) is not part of lens design, WAVE designers consider it critical; thus,, TLT at four places was also compared, revealing high consistency across most positions.
Statistical analysis
All statistical analyses were performed using SPSS version 27.0 (SPSS, Inc., Chicago, Illinois, USA). Descriptive statistics ( means and standard deviations or counts and percentages,as appropriate) were calculated.The normality of the data was assessed via Kolmogorov–Smirnov tests (P>0.05). Refractive sphere and cylinder (J0, J45), spherical equivalent refraction (SER), and axial length were compared before ortho-k treatment and after lens wear discontinuation using the paired t-test. The Pearson correlation coefficient was used to evaluate simple correlations between Rwo and Rwith, with best fitting lines added for both. The consistence of these lines was compared to intuitively reflect consistency between Rwo and Rwith. Intraclass correlation coefficients (ICCs) and their 95% confidence intervals were calculated for lens parameters from both software packages, with an ICC cut-off point of 0.85 considered acceptable. Bland and Altman analyses were also performed, including calculation of the mean difference (MD) between baseline and post-discontinuation conditions, the standard deviation (SD) of MD, and the upper and lower 95% limits of agreement (95% LoA). A two-tailed P<0.05 was considered statistically significant.
RESULTS
The change of spherical, cylindrical refractive components, and axial length
Before ortho-k treatment, the spherical and cylindrical refractive components were as follows: J0 was -2.80 ± 1.17 DS (range, −5.50 to -0.50 DS) , J45 was 0.21 ± 0.56 DC (range, −0.73 to 2.00 DC) and the clindrical refractive error was -0.19 ± 0.53 DC (range, −1.99 to −0.53 DC). After at least one year of ortho-k treatment followed by 1 to 2 months of lens wear discontinuation, these values changed significantly: J0 shifted to −3.37 ± 1.26 DS (range, −7.00 to −1.00 DS, P<0.001) , J45 to −0.04 ± 0.24 DC (range, −0.63 to 0.80 DC, P=0.03), and the cylindrical refractive error to 0.02 ± 0.31 DC (range, −0.96 to 0.84 DC, P=0.04) . Additionally, axial length (AL) increased from 24.71 ± 0.88 mm (range, 22.96 to 26.72 DS) to 25.12 ± 0.82 mm (range, 23.07 to 27.00 mm, P<0.001). Both the change in AL and the spherical refractive error were statistically significant (Supplemental Table 1).
Consistency of Rwo and Rwith by simulating the condition of baseline and after lens wear discontinuation respectively
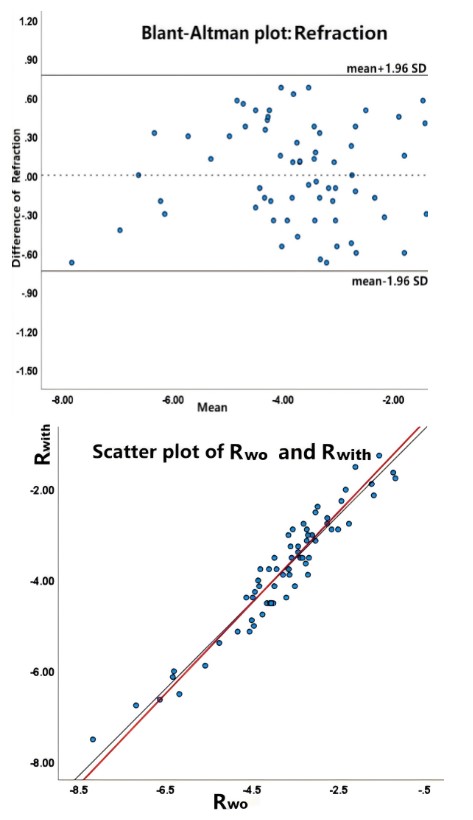
As shown in Figure 3b, a linear relationship exists between Rwo and Rwith (r=0.96; P<0.001). Following short-term discontinuation of ortho-k treatment, the mean Rwith was measured at (-3.68 ± 1.29) D (P<0.001). The average Rwo, calculated using our refractive formula prior ortho-k treatment, was (-3.76 ± 1.34) D, with a mean difference of (-0.02 ± 0.38) D between two methods, a difference that was statistically insignificant (P=0.92). Figure 3 demonstrates a high degree of agreement between the two methods, with data points randomly distributed around the line of equality, indicating no systematic bias. Furthermore, a high intraclass correlation was observed (ICC=0.96, P< 0.001), though this result was not explicitly shown in the figure. The Bland-Altman plot ( Figure 3a) illustrates the differences in refraction against the mean values, with the upper and lower limits of agreement (± 1.96 SD) clearly marked. The 95% limits of agreement between Rwo and Rwith were not clinically significant, confirming strong methodological consistency.
Comparison of Lens parameters generated by Easyfit software at the simulated condition of baseline and after lens wear discontinuation
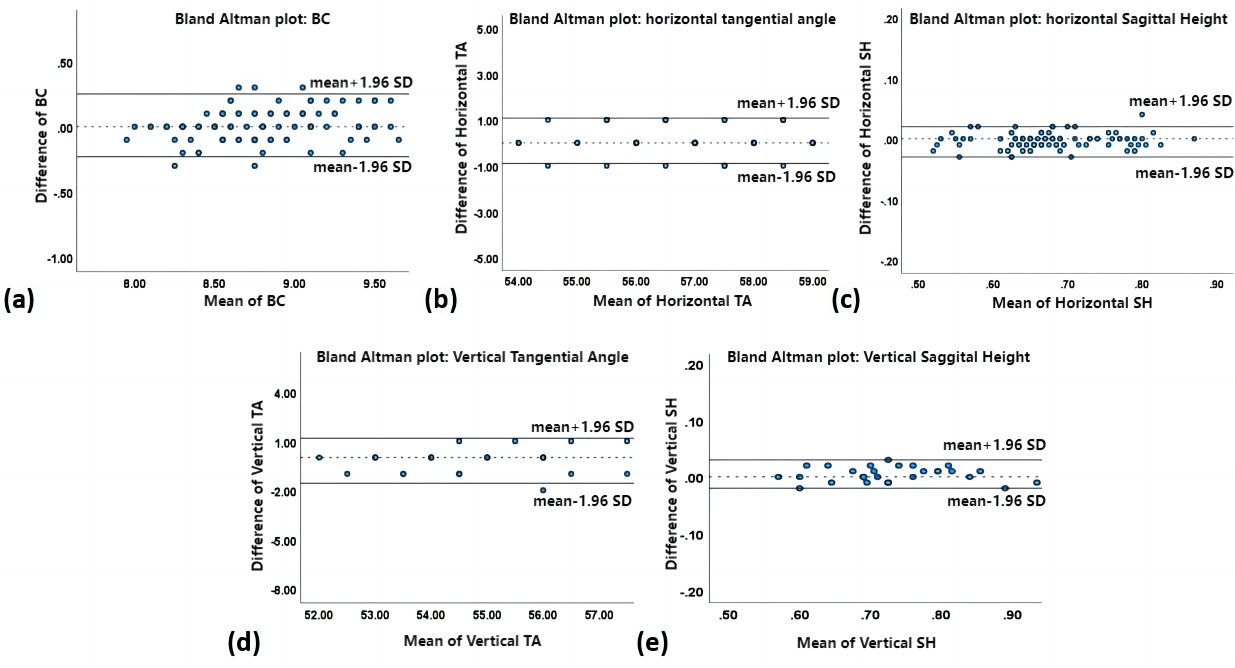
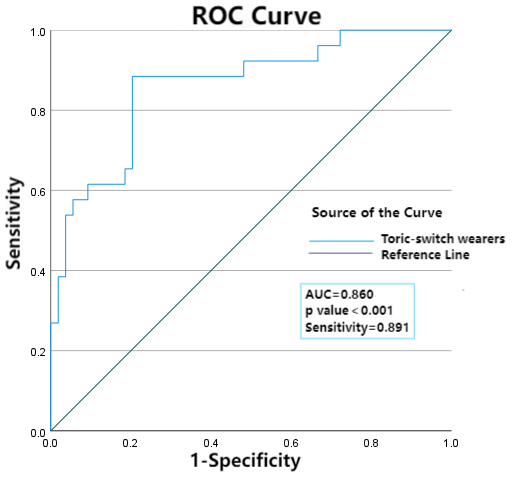
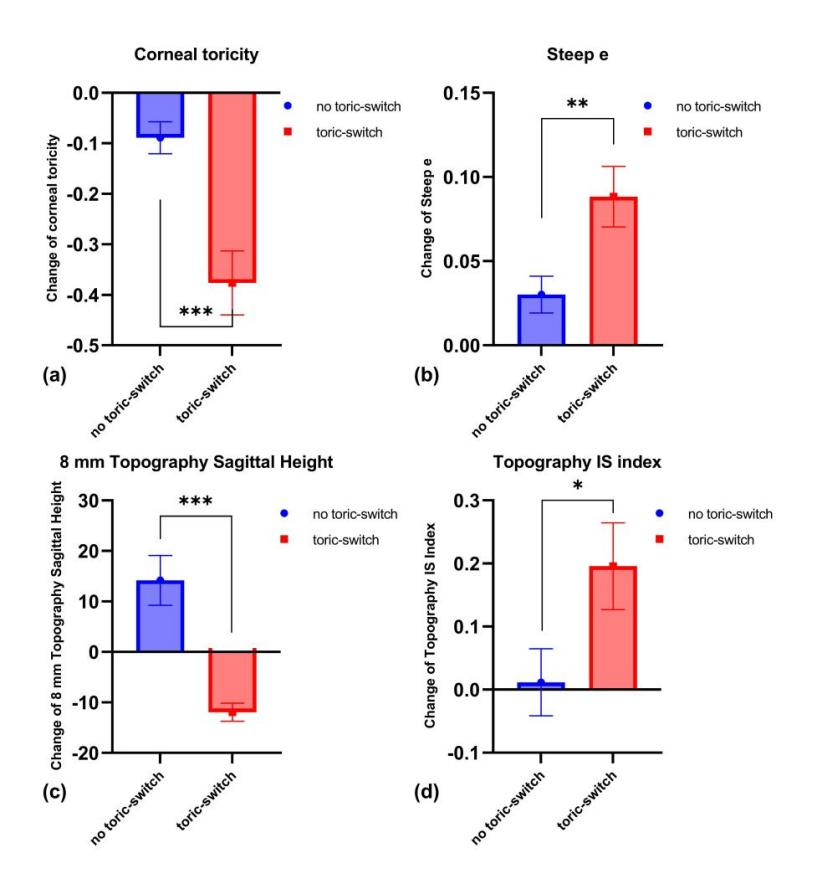
After importing the baseline corneal topography with Rwo, the software immediately generated recommended lens parameters, simulating the condition of "reorder without lens wear discontinuation". The reorder procedure following lens wear discontinuation followed a similar workflow, requiring the import of new baseline topography and Rwith. The generated lens parameters were subsequently compared, and the ICC results are presented in Table 2. The first generated parameter was the lens design type, which determined whether a toric design was required. If a toric design was recommended, two additional parameters (Vertical TA and SH) were generated. Notably, a significant shift in lens design occurred under the simulated condition of lens wear discontinuation. Based on post-discontinuation topography, 46 and 48 cases required spherical and toric design, respectively, compared to 64 spherical and 30 toric designs using baseline topography. Consequently, the software automatically switched 37.5% of the patients to toric design. The ROC curve analysis revealed that diagnostic performance was optimized when combining multiple baseline variables, with the area under the ROC curve (AUC) reaching 0.86 for the combined model (Supplemental Figure 2). Topographic parameters showing significant differences before and after lens wear discontinuation among patients recommended for a toric design switch are detailed in Supplemental Figure 3. These included corneal toricity, Steep e, 8 mm Topography Sagittal Height, and IS Index, all of which exhibited significant changes. Additional lens parameters were also generated, and as shown in Table 2, high ICC values were observed across all measurements. All ICC values exceeded 0.90, which the Vertical Sagittal Height demonstrating the highest correlation (ICC=0.99, P<0.001). As anticipated, the differences in all lens parameters between baseline and post-discontinuation conditions were minimal and statistically insignificant (all P>0.05).The Bland-Altman plots (Figure 4) further confirmed excellent agreement between two simulated conditions, with no clinically significant differences observed.
Comparison of lens parameters generated by WAVE software at the simulated condition of baseline and post-discontinuation
Although the appropriate lens designs differ between the two software programs, the procedures for importing topography data along with corresponding refraction information to generate lens parameters under different conditions using WAVE software are similar to those in Easyfit software. The ICC values for Lens SAG and Tear LT are presented in Table 2.
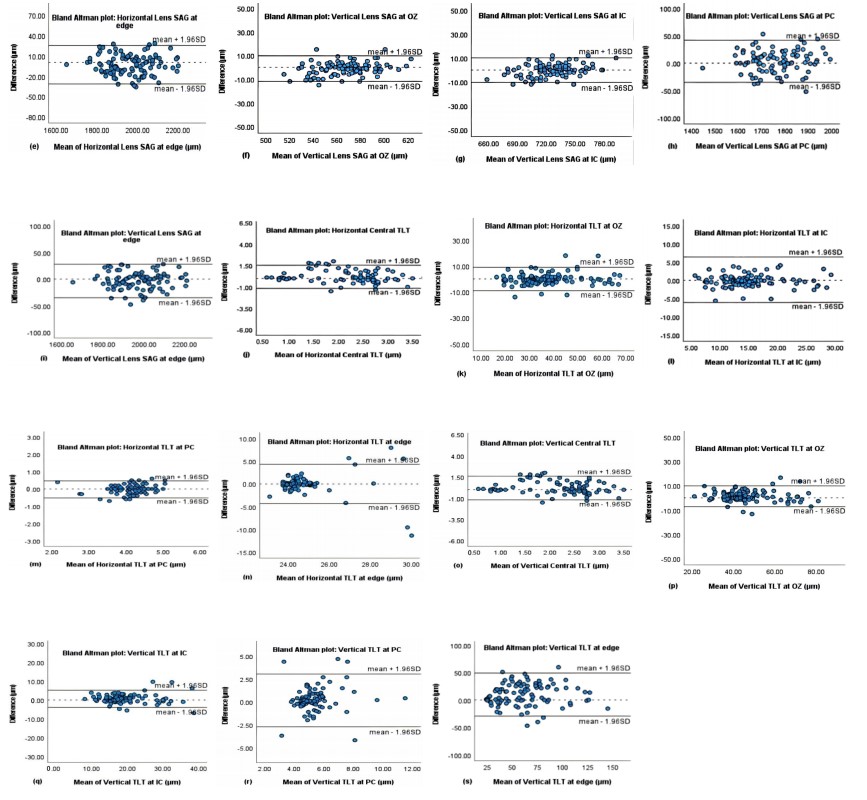
Although WAVE software was not constrained to specific positions at 8 semi-meridians, this trail achieved very high intraclass reliability ( with ICC values of 0.987 and 0.981 for horizontal and vertical Lens SAG at the edge, respectively, both P<0.001). Similarly, the ICC value for the BC was also high and even higher than that obtained with Easyfit software. All the Lens SAG values at different positions in our analysis, which were based on baseline topography, were highly consistent with corresponding SAG values when topography data was imported after discontinuing lens wear. Surprisingly, not only the Lens SAG values but also TLT values at some positions exhibited high ICC values between two conditions. Along both horizontal and vertical meridians, the TLT values at OZ and IC showed high consistency ( with ICC values of 0.951 and 0.935 for horizontal and vertical TLT at IC, respectively, both P<0.001), except for the SAG values at the PC and the edge, with had relatively low ICC values. Bland–Altman plots of lens parameters in WAVE software, along with the 95% limits of agreement (LoA), are also shown in Figure 5. The LoA for Lens SAGs at different positions along both horizontal and vertical meridians were mostly within the 95% LoA. Regarding TLT, the LoAs at PC and edge were nearly all within the 95% LoA, while the LoAs at OZ and IC were outside the maximum tolerated difference. Both ICC values and Bland–Altman plots indicate a rather high consistency of lens parameters between the two simulated conditions in WAVE software, based on the import of corresponding topography data with refraction information.
DISCUSSION
Few studies have reported on whether new lens can be directly reordered using software without the need for short-term discontinuation of lens wear.[13, 20] In the current study, we first assessed the feasibility of the software-based ortho-k lens system in directly reordering new lenses by utilizing baseline corneal topography, without the requiring patients to discontinue lens wear. Moreover, the two software programs used in this trial are designed for lens types: one for three-curve lenses and the other for VST-like ortho-k lenses, which represent the two most commonly used lenses types in the international market.
Currently, in the field of optometry research, the integration of Artificial Intelligence (AI) with myopia diagnosis and treatment is gaining popularity.[22] AI has been combined with retinal fundus photographs to enable earlier diagnosis of myopia, estimate approximate refraction values, and predict increase in axial length.[23, 24] Consequently, a new lens-ordering method assisted by software without the need for diagnostic fitting trials has emerged. This method has improved the efficiency of lens fitting,increasing the first-time successful fitting rate and saving more time for patients.[15] For example, Easyfit software, originally designed for the NKL lens brand (which has a three-curve design similar to CRT model), and WAVE software, which supports the WAVE lens brand with the characteristic four-zone VST-like model, are both popular due to their ability to simulate the lens-fitting state. Many studies have demonstrated that the clinical effects obtained using software are the same as those achieved through standard methods.[18, 25] However, the software-based approach mainly offers convenience for the first-time lens wearers; yet, no studies have taken this into consideration and addressed this question.
At the simulated condition where lens wear is not discontinued, and based on baseline topography, the calculation of Rwo is another vital step, as it is essential for generating lens parameters. Since the target refraction is related to the selection of BC, which can significantly impact the overall corneal topography, it is vital to accurately predict Rwo.[20] In the study by Li, et al.,[20] after incorporating refraction data, the accuracy of predicted K values (K1 and K2) when reordering new lenses in their optimal model was improved to a certain extent. In this study, the excellent fitting curve indicated that Rwo is highly consistent with Rwith after 1-2 months of lens wear discontinuation (ICC=0.96). Moreover, the minimal differences (within ± 0.7 diopter) also suggest a high accuracy of Rwo and the feasibility of the empirical formula. In summary, the empirical formula used to predict the myopia progression in ortho-k wearers in clinical practice is reliable and practical.
Notably, the lens parameters generated by Easyfit software under the condition of baseline and after lens wear discontinuation are highly consistent, with no significant difference between two conditions (Table 2 and Figure 4). Therefore, this demonstrates that for the three-curve model designed by Easyfit software, it is unreasonable to consider the lens parameters between two conditions as different. The high consistency of all lens parameters implies that importing baseline topography without the need for short-term wear discontinuation is entirely feasible, given the software's high successful fitting rate. Bland-Altman plots also showed that there was no statistically significant difference and high level of agreement was achieved between the two simulated conditions. Furthermore, according to clinical fitting experience and industry standards, we defined clinically meaningful difference thresholds for key lens parameters. Differences in BC exceeding 0.05 mm may significantly alter the central corneal flattening efficacy differences in SH >0.02 mm could lead to increased higher-order aberrations, and differences in TA >1 degree may affect lens centration. Therefore, Bland-Altman analysis for Easyfit in this study demonstrated that the 95% LoA for key lens parameters were below these thresholds, indicating that the discrepancies between the two methods were within clinically acceptable ranges. However, the lens type recommended by Easyfit software differed between the two conditions, with 37.5% of originally spheric design being switched to toric design. By comparing the changes in topography parameters before and after ortho-k lens discontinuation between the two conditions, several key parameters that influence lens type design were identified (Supplemental Figure 3). The toric-switch group was characterised by a significant increase in corneal toricity and significant decrease in the Steep e and IS index after lens wear discontinuation Regarding 8 mm topography sagittal height, it significantly increased in toric-switch wearers but decreased in others. All four parameters are mainly related to corneal morphology, so their changes reflect that the corneal shape of toric-switch wearers became more asymmetric, irregular and steep, especially along the vertical meridian. Indeed, several studies have reported differences in corneal and topographic changes between baseline and after lens wear discontinuation.[11, 26-28] These changes may be responsible for the switch to toric lens design. However, the ROC curve with a relatively high AUC (with value of 0.86) in the predicted model demonstrated that it could achieve the highest success rate when most baseline parameters were combined to diagnose these patients. Therefore, when using Easyfit software to reorder NKL or other three-curve lenses such as CRT, it is necessary to carefully evaluate the characteristics of wearers’ corneal topography and combine their baseline information to make a correct choice in final lens type. Chen, et al.[9] mentioned that some subjects required toric lenses to maintain good lens centration and visual correction when being refitted with ortho-k lenses after lens wear discontinuation, but they provided opinion on lens adjustment based on topography after short-term discontinuation and did not indicate whether lens wear should be stopped before reordering. Although many optometry centers and optometrists empirically reorder ortho-k lens for these patients without requiring lens wear discontinuation, there is no theoretical support and verification to guarantee the suitability of new lenses.[15] Therefore, this study provides strong theoretical support to verify that it is feasible to reorder lens with the assistance of software without the need for short-term lens wear discontinuation. In conclusion, it is feasible to directly reorder new NKL lens based on Easyfit software without discontinuing lens wear.
In addition, the VST design implemented with the WAVE system also demonstrated high consistency. As can be seen from Table 2 and Figure 5, the BC, Lens SAG at four positions (OZ, IC, PC and edge) along both horizontal and vertical meridians clearly show almost no bias between lens parameters under the two simulated conditions. The high ICC values for these lens parameters indicate that using baseline data directly when reordering new lenses is highly reliable and practical, with minimal variability. Although the ICC has been criticized for being a dimensionless value, the results obtained from the WAVE software are robust enough to suggest consistency between two conditions. Since more SAG generates more mechanical force, a tendency can be observed: the Lens SAG decreased along the horizontal meridian while vertical SAG increased after discontinuing lens wear. Both of these changes may have an impact on corneal curvature alternation. Although the relevant changes were insignificant in our study, they could potentially causes physiological consequences if they reach a sufficient magnitude or persist for a sufficient duration.[29] Fortunately, what is certain is that these changes imply an increase in corneal toricity and a gradually compromised lens fit. Consequently, these parameters may be more useful as they can be readily and easily interpreted in a meaningful way in clinical setting. Moreover, the plots also reveal that the distinction in TLT between two conditions increases with the distance of a given position from tear layer center. Specifically, high consistency is achieved in TLT at the OZ and IC positions, while low consistency is observed at the PC and lens edge positions along both horizontal and vertical meridians. We believe that the discrepancies at different positions may be due to the compensatory effect of the lens SAG at corresponding positions.[7] It is well-known that the external force generated by an ortho-k lens during nighttime wear depends not only on the mechanical pressure of the lens but also on the hydraulic pressure of tears. Both forces act on the cornea to reshape and flatten it.[29] Corresponding to the increased corneal toricity during long-term wear, all the horizontal and vertical TLT decreased at the four positions exhibited similar changes. Specifically, the vertical TLT increased while horizontal TLT decreased after short-term lens wear discontinuation. This can be explained by the fact that a thicker TLT exerts more pressure on cornea, leading to a shift in corneal morphology and curvature towards a steeper direction. Conversely, the horizontal TLT thins, and FK becomes flatter. Fortunately, the TLT at different positions are not lens parameters and do not affect the final conclusion. According to the Bland-Altman analyses of the lens parameters for WAVE system, the 95% LoA for the Lens SAGs LoA at different positions along both horizontal and vertical meridians were mostly within the 95% LoA. Similarly, based on clinical fitting experience, clinically significant difference thresholds for key parameters of VST-based lens were also defined. Differences in BC < 0.2 mm are considered tolerable, while differences in both the horizontal and vertical Lens SAG at the OZ < 20 μm are considered acceptable. Moreover, differences in both horizontal and vertical Lens SAG at the IC < 30 μm are considered tolerable. Therefore, the Bland-Altman analysis for the WAVE demonstrated that the 95% LoA for most of the key lens parameters fell below clinical thresholds, indicating that there are no clinically siginificant discrepancies between two methods. By importing baseline topography with Rwo and topography after lens wear discontinuation with Rwith respectively, it is considered that within the tolerance range of WAVE software, reordering WAVE lenses and possibly other VST-based lens brands without the need to discontinue lens wear is feasible.
However, the study also has several limitations. First, the software algorithms demand that all input topography data to be of high quality, which requires patients to be highly cooperative. Since most patients are children and tend to be difficult to cooperate, this method cannot be recommended for all patients. The first-fit success rate decreases when using low-quality maps. If the scan quality is poor, the Easyfit software shows no response, while the WAVE software recommends repeating the scans. Second, the users of lens design software are responsible for ensuring that the data entered into the software is accurate and complete. This requires them to be proficient in software operation and meticulous when importing data. Furthermore, not only topography but also target refraction plays an important role in software-based lens design. Therefore, it is extremely essential that Rwo, calculated by our formula, is highly consistent with Rwith. Based on our well-established formula, which has demonstrated excellent performance in predicting Rwo after long-term lens wear, we can reorder ortho-k lenses for these patients with a high success rate. Next, the software used in this study only covers two brands, representing the design of three-curve and four-zone reverse geometry lens respectively. However, as more and more lens design software are being developed in the global market, relying solely on two predominant software makes it difficult to verify and represent all types of ortho-k lenses. It is advisable to explore more popular software to evaluate their suitability. Moreover, although a broad age range (8–45 years) and spherical refractive error range (-0.50 to -6.50 D) were included, the sample size (n=94) was insufficient to support subgroup analyses stratified by age or refraction. Future studies should expand the sample size or adopt multicenter designs to validate findings across different subgroups. No a priori sample size calculation was performed, which may have compromised statistical power. Subsequent research should calculate the required sample size based on the effect size. Finally, we analyzed the clinical data of patients without information about their actual lens wear fitting separately. According to the impact of ortho-k lens on the ocular surface, microscopic examination revealed evidence of corneal staining and microcysts in many subjects. All cases were graded as I or II according to the Efron scale, and most patients had no conscious symptoms. However, the evaluations of the ocular surface status after ortho-k treatment were incomplete, so the incidence of relevant side effect could not be calculated. In the future, it is necessary to conduct a prospective study and pay attention to the response of lens wearers to the reordered lens designed by software, as it is unrealistic to compare the performance of new lens using topograghy after lens wear discontinuation with Rwith and baseline topograghy with Rwo.
In conclusion, it is certainly feasible to directly reorder new lenses using baseline corneal topography without discontinuing lens wear by using software-based system. This study demonstrated that the Easyfit software, a computer-assisted system for NKL lens and possibly other three-curve design, as well as the WAVE software, a diagnostic lens set for WAVE lens and potentially VST-designed brands, are capable of facilitating lenses reordering for ortho-k lens wearers. The results showed a high consistency between all software-generated lens parameters and Rwith or Rwo. In other words, it is feasible to directly reorder new ortho-k lenses without discontinuing lens wear based on Easyfit and WAVE software,and this is within the tolerance range of their programs. The significant time-saving benefit is clinically meaningful, bringing convenience to both lens wearers and optometrists. In the future, the feasibility of using baseline to
pography to directly reorder new lenses for required wearers needs to be clinically validated.
Figure 1 Flow diagram illustrating the participants’ enrolment and study design
Figure 2 Research framework and data processing of the current study
Figure 3 Correlation of Rwo via empirical formula and Rwith after discontinuation of lens wear
(a) Bland-Altman analysis of our study relation of Rwo via empirical formula and Rwith after lens weardiscontinuation. (b) Scatter plot of Rwovia empirical formula and Rwith after lens weardiscontinuation.Red line refers to reference (Y=X), Black line refers to fitted formula of refraction (Y=0.96X + 0.12).
Figure 4 Bland-Altman plots for lens parameters generated by Easyfit Software at two conditions
(a) BC (b) horizontal TA (c) horizontal SH (d) vertical TA (e) vertical SH.
Abbreviations: BC, base curve; Horizontal TA, horizontal tangential angle; Horizontal SH, horizontal sagittal height; Vertical TA, vertical tangential angle; Vertical SH, vertical sagittal height.
Figure 5 Bland-Altman plots for lens parameters generated by WAVE Software at two conditions
(a) BC (b) Horizontal Lens SAG at IC (c) Horizontal Lens SAG at PC (d) Horizontal Lens SAG at OZ (e) Horizontal Lens SAG at edge (f) Vertical Lens SAG at OZ (g) Vertical Lens SAG at IC (h) Vertical Lens SAG at PC (i) Vertical Lens SAG at edge (j) Horizontal Central TLT (k) Horizontal TLT at OZ (l) Horizontal TLT at IC (m) Horizontal TLT at PC (n) Horizontal TLT at edge (o) Vertical Central TLT (p) Vertical TLT at OZ (q) Vertical TLT at IC (r) Vertical TLT at PC (s) Vertical TLT at edge.
Table 1 Statistical characteristics of the baseline data
Supplemental Figure 1 Lens parameters generated on two computer-assisted lens design software
The upper part is the WAVE lens brand designed by WAVE, while the lower part is the NKL or CRT-like ortho-k designed by Easyfit.
Abbreviations: BC, base curve; Horizontal TA, horizontal tangential angle; Horizontal SH, horizontal sagittal height; Vertical TA, vertical tangential angle; Vertical SH, vertical sagittal height; RZD, reverse zone depth; TLT, tear layer thickness; Lens SAG, lens sagittal depth; OZ, back optic zone; IC, intermediate curve; PC, peripheral curve; Edge, edge lift.
Supplemental Figure 2 Receiver operating characteristics (ROC) curve of multiple combined baseline indicators for ortho-k lens wearers
Supplemental Figure 3 Changes of topographic parameters bewteen baseline and after discontinuation that were significantly different in toric-switch group and no toric-switch group
(a) Topography toricity (b) Steep e (c) 8 mm Topography Sagittal Height (d) Topography IS Index.
Abbreviations: Toricity, corneal astigmatism; Steep e, steep eccentricity; Topography IS Index, inferior-superior index of the topography.
Supplemental Table 1 Changes of Subjective Refractive Errors and Axial Length during the period of ortho-k treatment and after 1-2 months lens wear discontinuation
J0 =−C cos 2θ/2; J45 =−C sin 2θ/2 (θ: Refractive astigmatism axis)
Notes: J0 =−C cos 2θ/2; J45 =−C sin 2θ/2 (θ: Refractive astigmatism axis). *Denotes a paired t test. Data are presented as mean ± SD (standard deviation).
(Ⅰ) Conception and design: Mingxin Lu, Jinyun Jiang
(Ⅱ) Administrative support: Shengsong Xu, Xiao Yang
(Ⅲ) Provision of study materials or patients:Hongmei Tan, Weiyin Chen, Cong Li
(Ⅳ) Collection and assembly of data: Mingxin Lu
(Ⅴ) Data analysis and interpretation: Mingxin Lu
(Ⅵ) Manuscript writing: All authors
(Ⅶ) Final approval of manuscript: All authors
Funding
This work was supported by the National Natural Science Foundation of China (82371089).
Conflict of Interests
None of the authors has any conflicts of interest to disclose. All authors have declared in the completed the ICMJE uniform disclosure form. Feasibility of utilizing a software-based fitting system for orthokeratology lens recordering without short-term discontinuation of lens wear Mingxin Lu, et al. 259
Patient Consent for Publication
None
Ethical Statement
The current study was conducted at Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangzhou, China. This study adhered to the tenets of the Declaration of Helsinki of 1964 and its later amendments. This study was approved by the Institutional Ethical Committee of Zhongshan Ophthalmic Center, Sun Yat-Sen University (L2019104).
Provenance and Peer Review
This article was a standard submission to our journal. The article has undergone peer review with our anonymous review system.
Data Sharing Statement
None
Open Access Statement
This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication
through the relevant DOI and the license).
1、Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016, 123(5): 1036-1042. DOI: 10.1016/j.ophtha.2016.01.006. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016, 123(5): 1036-1042. DOI: 10.1016/j.ophtha.2016.01.006.
2、Kang HM, Lee CS, Park HJ, et al. Characteristics of rhegmatogenous retinal detachment after refractive surgery: comparison with myopic eyes with retinal detachment. Am J Ophthalmol. 2014, 157(3): 666-672.e1-2. DOI: 10.1016/j.ajo.2013.12.004. Kang HM, Lee CS, Park HJ, et al. Characteristics of rhegmatogenous retinal detachment after refractive surgery: comparison with myopic eyes with retinal detachment. Am J Ophthalmol. 2014, 157(3): 666-672.e1-2. DOI: 10.1016/j.ajo.2013.12.004.
3、Moriyama M, Ohno-Matsui K, Shimada N, et al. Correlation between visual prognosis and fundus autofluorescence and optical coherence tomographic findings in highly myopic eyes with submacular hemorrhage and without choroidal neovascularization. Retina. 2011, 31(1): 74-80. DOI: 10.1097/IAE.0b013e3181e91148. Moriyama M, Ohno-Matsui K, Shimada N, et al. Correlation between visual prognosis and fundus autofluorescence and optical coherence tomographic findings in highly myopic eyes with submacular hemorrhage and without choroidal neovascularization. Retina. 2011, 31(1): 74-80. DOI: 10.1097/IAE.0b013e3181e91148.
4、Mateo C, Dutra Medeiros M, Alkabes M, et al. Illuminated Ando plombe for optimal positioning in highly myopic eyes with vitreoretinal diseases secondary to posterior staphyloma. JAMA Ophthalmol. 2013, 131(10): 1359-1362. DOI: 10.1001/jamaophthalmol.2013.4558. Mateo C, Dutra Medeiros M, Alkabes M, et al. Illuminated Ando plombe for optimal positioning in highly myopic eyes with vitreoretinal diseases secondary to posterior staphyloma. JAMA Ophthalmol. 2013, 131(10): 1359-1362. DOI: 10.1001/jamaophthalmol.2013.4558.
5、Cho P, Cheung SW. Retardation of myopia in orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012, 53(11): 7077. DOI: 10.1167/iovs.12-10565. Cho P, Cheung SW. Retardation of myopia in orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012, 53(11): 7077. DOI: 10.1167/iovs.12-10565.
6、 Hiraoka T, Kakita T, Okamoto F, et al. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest Ophthalmol Vis Sci. 2012, 53(7): 3913-3919. DOI: 10.1167/iovs.11-8453. Hiraoka T, Kakita T, Okamoto F, et al. Long-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up study. Invest Ophthalmol Vis Sci. 2012, 53(7): 3913-3919. DOI: 10.1167/iovs.11-8453.
7、Nichols JJ, Marsich MM, Nguyen M, et al. Overnight orthokeratology. Optom Vis Sci. 2000, 77(5): 252-259. DOI: 10.1097/00006324-200005000-00012. Nichols JJ, Marsich MM, Nguyen M, et al. Overnight orthokeratology. Optom Vis Sci. 2000, 77(5): 252-259. DOI: 10.1097/00006324-200005000-00012.
8、Si JK, Tang K, Bi HS, et al. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015, 92(3): 252-257. DOI: 10.1097/OPX.0000000000000505. Si JK, Tang K, Bi HS, et al. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015, 92(3): 252-257. DOI: 10.1097/OPX.0000000000000505.
10、Ma L, Xu M, Wang J, et al. Analysis of the reasons for the discontinuation of orthokeratology lens use: a 4-year retrospective study. Eye Contact Lens. 2022, 48(8): 335-339. DOI: 10.1097/ICL.0000000000000910. Ma L, Xu M, Wang J, et al. Analysis of the reasons for the discontinuation of orthokeratology lens use: a 4-year retrospective study. Eye Contact Lens. 2022, 48(8): 335-339. DOI: 10.1097/ICL.0000000000000910.
11、Santodomingo-Rubido J, Villa-Collar C, Gilmartin B, et al. Short-term changes in ocular biometry and refraction after discontinuation of long-term orthokeratology. Eye Contact Lens. 2014, 40(2): 84-90. DOI: 10.1097/ICL.0000000000000014.Santodomingo-Rubido J, Villa-Collar C, Gilmartin B, et al. Short-term changes in ocular biometry and refraction after discontinuation of long-term orthokeratology. Eye Contact Lens. 2014, 40(2): 84-90. DOI: 10.1097/ICL.0000000000000014.
12、Zhu Q, Yin J, Li X, et al. Effects of long-term wear and discontinuation of orthokeratology lenses on the eyeball parameters in children with myopia. Int J Med Sci. 2023, 20(1): 50-56. DOI: 10.7150/ijms.79496. Zhu Q, Yin J, Li X, et al. Effects of long-term wear and discontinuation of orthokeratology lenses on the eyeball parameters in children with myopia. Int J Med Sci. 2023, 20(1): 50-56. DOI: 10.7150/ijms.79496.
13、Fan Y, Yu Z, Peng Z, et al. Machine learning based strategy surpasses the traditional method for selecting the first trial Lens parameters for corneal refractive therapy in Chinese adolescents with myopia. Contact Lens Anterior Eye. 2021, 44(3): 101330. DOI: 10.1016/j.clae.2020.05.001. Fan Y, Yu Z, Peng Z, et al. Machine learning based strategy surpasses the traditional method for selecting the first trial Lens parameters for corneal refractive therapy in Chinese adolescents with myopia. Contact Lens Anterior Eye. 2021, 44(3): 101330. DOI: 10.1016/j.clae.2020.05.001.
14、Fan Y, Yu Z, Tang T, et al. Machine learning algorithm improves accuracy of ortho-K lens fitting in vision shaping treatment. Contact Lens Anterior Eye. 2022, 45(3): 101474. DOI: 10.1016/j.clae.2021.101474. Fan Y, Yu Z, Tang T, et al. Machine learning algorithm improves accuracy of ortho-K lens fitting in vision shaping treatment. Contact Lens Anterior Eye. 2022, 45(3): 101474. DOI: 10.1016/j.clae.2021.101474.
15、Chan KY, Cheung SW, Cho P. Clinical performance of an orthokeratology lens fitted with the aid of a computer software in Chinese children. Cont Lens Anterior Eye. 2012, 35(4): 180-184. DOI: 10.1016/j.clae.2012.01.004. Chan KY, Cheung SW, Cho P. Clinical performance of an orthokeratology lens fitted with the aid of a computer software in Chinese children. Cont Lens Anterior Eye. 2012, 35(4): 180-184. DOI: 10.1016/j.clae.2012.01.004.
16、Lu D, Gu T, Lin W, et al. Efficacy of trial fitting and software fitting for orthokeratology lens: one-year follow-up study. Eye Contact Lens. 2018, 44(5): 339-343. DOI: 10.1097/ICL.0000000000000539. Lu D, Gu T, Lin W, et al. Efficacy of trial fitting and software fitting for orthokeratology lens: one-year follow-up study. Eye Contact Lens. 2018, 44(5): 339-343. DOI: 10.1097/ICL.0000000000000539.
17、 Verkicharla PK, Kammari P, Das AV. Myopia progression varies with age and severity of myopia. PLoS One. 2020, 15(11): e0241759. DOI: 10.1371/journal.pone.0241759. Verkicharla PK, Kammari P, Das AV. Myopia progression varies with age and severity of myopia. PLoS One. 2020, 15(11): e0241759. DOI: 10.1371/journal.pone.0241759.
18、Wu R, Stapleton F, Swarbrick HA. Residual corneal flattening after discontinuation of long-term orthokeratology lens wear in Asian children. Eye Contact Lens. 2009, 35(6): 333-337. DOI: 10.1097/ICL.0b013e3181bdc41f. Wu R, Stapleton F, Swarbrick HA. Residual corneal flattening after discontinuation of long-term orthokeratology lens wear in Asian children. Eye Contact Lens. 2009, 35(6): 333-337. DOI: 10.1097/ICL.0b013e3181bdc41f.
19、Zhang L, Zhang Y, Liu Y, et al. A novel fitting algorithm for alignment curve radius estimation using corneal elevation data in orthokeratology lens trial. Cont Lens Anterior Eye. 2017, 40(6): 401-407. DOI: 10.1016/j.clae.2017.09.018. Zhang L, Zhang Y, Liu Y, et al. A novel fitting algorithm for alignment curve radius estimation using corneal elevation data in orthokeratology lens trial. Cont Lens Anterior Eye. 2017, 40(6): 401-407. DOI: 10.1016/j.clae.2017.09.018.
20、Li Y, Zhao H, Fan Y, et al. A machine learning-based algorithm for estimating the original corneal curvature based on corneal topography after orthokeratology. Contact Lens Anterior Eye. 2023, 46(4): 101862. DOI: 10.1016/j.clae.2023.101862. Li Y, Zhao H, Fan Y, et al. A machine learning-based algorithm for estimating the original corneal curvature based on corneal topography after orthokeratology. Contact Lens Anterior Eye. 2023, 46(4): 101862. DOI: 10.1016/j.clae.2023.101862.
21、Jones LA, Lynn Mitchell G, Mutti DO, et al. Comparison of ocular component growth curves among refractive error groups in children. Invest Ophthalmol Vis Sci. 2005, 46(7): 2317-2327. DOI: 10.1167/iovs.04-0945. Jones LA, Lynn Mitchell G, Mutti DO, et al. Comparison of ocular component growth curves among refractive error groups in children. Invest Ophthalmol Vis Sci. 2005, 46(7): 2317-2327. DOI: 10.1167/iovs.04-0945.
22、Zhang C, Zhao J, Zhu Z, et al. Applications of artificial intelligence in myopia: current and future directions. Front Med (Lausanne), 2022, 9: 840498. DOI: 10.3389/fmed.2022.840498. Zhang C, Zhao J, Zhu Z, et al. Applications of artificial intelligence in myopia: current and future directions. Front Med (Lausanne), 2022, 9: 840498. DOI: 10.3389/fmed.2022.840498.
23、Tang T, Yu Z, Xu Q, et al. A machine learning-based algorithm used to estimate the physiological elongation of ocular axial length in myopic children. Eye Vis (Lond), 2020, 7: 50. DOI: 10.1186/s40662-020-00214-2. Tang T, Yu Z, Xu Q, et al. A machine learning-based algorithm used to estimate the physiological elongation of ocular axial length in myopic children. Eye Vis (Lond), 2020, 7: 50. DOI: 10.1186/s40662-020-00214-2.
24、Varadarajan AV, Poplin R, Blumer K, et al. Deep learning for predicting refractive error from retinal fundus images. Invest Ophthalmol Vis Sci. 2018, 59(7): 2861. DOI: 10.1167/iovs.18-23887. Varadarajan AV, Poplin R, Blumer K, et al. Deep learning for predicting refractive error from retinal fundus images. Invest Ophthalmol Vis Sci. 2018, 59(7): 2861. DOI: 10.1167/iovs.18-23887.
25、Zhen Y, Shen J, Wang W, et al. Evaluation of orthokeratology lens fitting assisted by sagittal height simulation software. Eye Contact Lens. 2022, 48(2): 78-82. DOI: 10.1097/ICL.0000000000000861. Zhen Y, Shen J, Wang W, et al. Evaluation of orthokeratology lens fitting assisted by sagittal height simulation software. Eye Contact Lens. 2022, 48(2): 78-82. DOI: 10.1097/ICL.0000000000000861.
26、Maseedupally V, Gifford P, Lum E, et al. Central and paracentral corneal curvature changes during orthokeratology. Optom Vis Sci. 2013, 90(11): 1249-1258. DOI: 10.1097/OPX.0000000000000039. Maseedupally V, Gifford P, Lum E, et al. Central and paracentral corneal curvature changes during orthokeratology. Optom Vis Sci. 2013, 90(11): 1249-1258. DOI: 10.1097/OPX.0000000000000039.
27、Tahhan N, Toit RD, Papas E, et al. Comparison of reverse-geometry lens designs for overnight orthokeratology. Optom Vis Sci. 2003, 80(12): 796-804. DOI: 10.1097/00006324-200312000-00009. Tahhan N, Toit RD, Papas E, et al. Comparison of reverse-geometry lens designs for overnight orthokeratology. Optom Vis Sci. 2003, 80(12): 796-804. DOI: 10.1097/00006324-200312000-00009.
28、Queirós A, Lopes-Ferreira D, Yeoh B, et al. Refractive, biometric and corneal topographic parameter changes during 12 months of orthokeratology. Clin Exp Optom. 2020, 103(4): 454-462. DOI: 10.1111/cxo.12976. Queirós A, Lopes-Ferreira D, Yeoh B, et al. Refractive, biometric and corneal topographic parameter changes during 12 months of orthokeratology. Clin Exp Optom. 2020, 103(4): 454-462. DOI: 10.1111/cxo.12976.
30、Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016, 123(5): 1036-1042. DOI: 10.1016/j.ophtha.2016.01.006.
1、This work was supported by the National Natural Science Foundation of China (82371089).This work was supported by the National Natural Science Foundation of China (82371089).
()